
Anal Fissure are caused by trauma to the anus and anal canal. The cause of the trauma usually is a bowel movement, and many people can remember the exact bowel movement during which their pain began.
Thank you for reading this post, don't forget to subscribe!The fissure may be caused by a hard stool or repeated episodes of diarrhea. Occasionally, the insertion of a rectal thermometer, enema tip, endoscope, or ultrasound probe (for examining the prostate gland) can result in sufficient trauma to produce a fissure. During childbirth, trauma to the perineum (the skin between the posterior vagina and the anus) may cause a tear that extends into the anoderm.
The most common location for an anal fissure in both men and women (90% of all fissures) is the midline posteriorly in the anal canal, the part of the anus nearest the spine. Fissures are more common posteriorly because of the configuration of the muscle that surrounds the anus.
This muscle complex, referred to as the external and internal anal sphincters, underlies and supports the anal canal. The sphincters are oval-shaped and are best supported at their sides and weakest posteriorly. When tears occur in the anoderm, therefore, they are more likely to be posterior. In women, there also is weak support for the anterior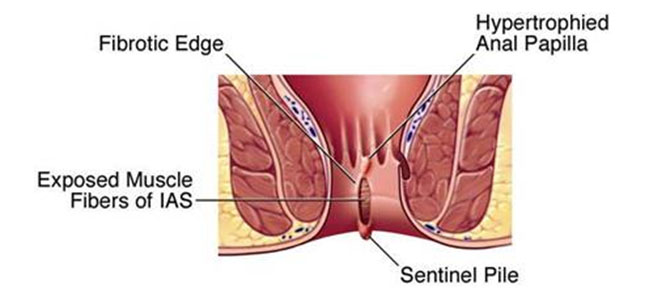 anal canal due to the presence of the vagina anterior to the anus. For this reason, 10% of fissures in women are anterior, while only 1% are anterior in men. At the lower end of fissures, a tag of skin may form, called a sentinel pile.
anal canal due to the presence of the vagina anterior to the anus. For this reason, 10% of fissures in women are anterior, while only 1% are anterior in men. At the lower end of fissures, a tag of skin may form, called a sentinel pile.
When fissures occur in locations other than the midline posteriorly or anteriorly, they should raise the suspicion that a problem other than trauma is the cause.
Other causes of fissures are anal cancer, Crohn’s disease, and leukemia as well as many infectious diseases including tuberculosis, viral infections (cytomegalovirus or herpes), syphilis, gonorrhea, Chlamydia, chancroid (Haemophilus ducreyi), and human immunodeficiency virus (HIV).
Among patients with Crohn’s disease, 4% will have an anal fissure as the first manifestation of their Crohn’s disease, and half of all patients with Crohn’s disease eventually will develop anal ulceration that may look like a fissure.
Studies of the anal canal in patients with anal fissures consistently show that the muscles surrounding the anal canal are contracting too strongly (they are in spasm), thereby generating a pressure in the canal that is abnormally high. The two muscles that surround the anal canal are the external anal sphincter and the internal anal sphincter.
The external anal sphincter is a voluntary (striated) muscle, that is, it can be controlled consciously. Thus, when we need to have a bowel movement we can either tighten the external sphincter and prevent the bowel movement, or we can relax it and allow the bowel movement.
On the other hand, the internal anal sphincter is an involuntary (smooth) muscle, that is, a muscle we cannot control. The internal sphincter is constantly contracted and normally prevents small amounts of stool from leaking from the rectum. When a substantial load of stool reaches the rectum, as it does just before a bowel movement, the internal anal sphincter relaxes automatically to let the stool pass (that is, unless the external anal sphincter is consciously tightened).
When an anal fissure is present, the internal anal sphincter is in spasm. In addition, after the sphincter finally does relax to allow a bowel movement to pass, instead of going back to its resting level of contraction and pressure, the internal anal sphincter contracts even more vigorously for a few seconds before it goes back to its elevated resting level of contraction.
It is thought that the high resting pressure and the “overshoot” contraction of the internal anal sphincter following a bowel movement pull the edges of the fissure apart and prevent the fissure from healing. The supply of blood to the anus and anal canal also may play a role in the poor healing of anal fissures.
Anatomic and microscopic studies of the anal canal on cadavers found that in 85% of individuals, the posterior part of the anal canal (where most fissures occur) has less blood flowing to it than the other parts of the anal canal. Moreover, ultrasound studies that measure the flow of blood showed that the posterior anal canal had less than half of the blood flow of other parts of the canal.
This relatively poor flow of blood is the main factor in preventing fissures from healing said Dr Qaisar Ahmed; It also is possible that the increased pressure in the anal canal due to spasms of the internal anal sphincter may compress the blood vessels of the anal canal and further reduce the flow of blood.
Symptoms of Anal Fissure
Patients with anal fissures almost always experience anal pain that worsens with bowel movements.
- The pain following a bowel movement may be brief or long-lasting; however, the pain usually subsides between bowel movements.
- The pain can be so severe that patients are unwilling to have a bowel movement, resulting in constipation and even fecal impaction. Moreover, constipation can result in the passage of a larger, harder stool that causes further trauma and makes the fissure worse.
- The pain also can affect urination by causing discomfort when urinating (dysuria), frequent urination, or the inability to urinate.
- Bleeding in small amounts, itching (pruritus ani), and a malodorous discharge may occur due to the discharge of pus from the fissure.
Diagnose Anal Fissure
A careful history usually suggests that an anal fissure is present, and a gentle inspection of the anus can confirm the presence of a fissure. If gentle eversion (pulling apart) of the edges of the anus by separating the buttocks does not reveal a fissure, a more vigorous examination following the application of a topical anesthetic to the anus and anal canal may be necessary. A cotton-tipped swab may be inserted into the anus to gently localize the source of the pain.
An acute anal fissure looks like a linear tear. A chronic anal fissure frequently is associated with a triad of findings that includes a tag of skin at the edge of the anus (sentinel pile), thickened edges of the fissure with muscle fibers of the internal sphincter visible at the base of the fissure, and an enlarged anal papilla at the upper end of the fissure in the anal canal.
If rectal bleeding is present, an endoscopic evaluation using a rigid or flexible viewing tube is necessary to exclude the possibility of a more serious disease of the anus and rectum. A sigmoidoscopy that examines only the distal part of the colon may be reasonable in patients younger than 50 years of age who have atypical anal fissure. In patients with a family history of colon cancer or age greater than 50 (and, therefore, at higher risk for colon cancer), a colonoscopy that examines the entire colon is recommended.
Atypical fissures that suggest the presence of other diseases, as discussed previously, require other diagnostic studies including colonoscopy and upper gastrointestinal (UGI) and small intestinal X-rays.
Allopathic remedies and OTC drugs for Anal Fissure
In allopathy, the goal of treatment for anal fissures is to break the cycle of spasms of the anal sphincter and its repeated tearing of the anoderm. In acute fissures, allopathic (nonoperative) therapy is successful in the majority of patients. Of acute fissures, 80% to 90% will heal with conservative measures as compared with chronic (recurrent) fissures, which show only a 40% rate of healing. Initial treatment involves adding bulk to the stool and softening the stool with psyllium or methylcellulose preparations and a high-fiber diet.
Sitz baths (essentially soaking in a tub of warm water). Sitz baths are encouraged, particularly after bowel movements, to relax the spasm, increase the flow of blood to the anus, and clean the anus without rubbing the irritated anoderm.
When there are enlarged internal hemorrhoids in addition to a fissure, the healing of the fissure is improved if the hemorrhoids are treated with sclerotherapy that shrinks them or with Homeopathic therapy that dissolves them, said Dr Qaisar Ahmed. After the application of a topical anesthetic, if a patient can tolerate a gentle examination of the rectum with a finger and an anoscope can be inserted through the anus, enlarged hemorrhoids can be identified, and if present, treated with sclerotherapy.
Prescription allopathic drugs
Anesthetics and steroids
Topical anesthetics (for example, xylocaine, lidocaine, tetracaine, and pramoxine) are recommended especially before a bowel movement to reduce the pain of defecation. Often, a steroid is combined with the anesthetic cream to reduce inflammation.
The use of steroids should be limited to two weeks because longer use will result in thinning of the anoderm (atrophy), which makes it more susceptible to trauma.
Oral allopathic medications to relax the smooth muscle of the internal sphincter have not been shown to aid any healing.
Nitroglycerin
Because of the possibility that spasms of the internal sphincter and reduced flow of blood to the sphincter play roles in the formation and healing of anal fissures, ointments with the muscle relaxant, nitroglycerin (glyceryl trinitrate), is effective in healing anal fissures.
Glycerin trinitrate (nitroglycerin) has been shown to cause relaxation of the internal anal sphincter and to decrease the anal resting pressure. When ointments containing nitroglycerin are applied to the anal canal, the nitroglycerin diffuses across the anoderm and relaxes the internal sphincter, and reduces the pressure in the anal canal. This relieves spasms of the muscle and also may increase the flow of blood, both of which promote the healing of fissures.
Unlike Nitropaste, a 2.0% concentration of nitroglycerin that is used on the skin for patients with heart disease and angina, the nitroglycerin ointment used for treating anal fissures contains a concentration of nitroglycerin of only 0.2%. The dose of nitroglycerin often is limited by side effects.
The usual side effects are low blood pressure, severe headaches (due to dilation of blood vessels in the head), dizziness or lightheadedness (due to a drop in blood pressure). Nitroglycerin is more rapidly absorbed if blood flow in the anoderm is high. For this reason, it is recommended that nitroglycerin not be applied within 30 minutes of a bath since the warm water of the bath enlarges (dilates) the blood vessels in the body and increases the flow of blood. Additionally, the first application of nitroglycerin should be at bedtime while the patient is lying down to prevent falls due to lightheadedness.
The side effects of nitroglycerin often are self-limited, that is, they become less with repeated use. If side effects are pronounced, nitroglycerin should be discontinued.
Drugs for impotence (for example, sildenafil (Viagra), should not be used together with nitroglycerin since they increase the risk of developing low blood pressure.
Calcium channel-blocking drugs (CCBs)
As is the case with nitroglycerin, ointments containing calcium channel-blocking drugs (for example, nifedipine or diltiazem) relax the muscles of the internal sphincter. They also expand the blood vessels of the anoderm and increase the flow of blood.
Nifedipine ointment (2%) is applied like nitroglycerin ointment. Healing of chronic fissures has been reported in up to 27% of patients treated with calcium channel blockers, they are most effective with acute fissures.
Botulinum toxin
Botulinum toxin (Botox) relaxes (actually paralyzes) muscles by preventing the release of acetylcholine from the nerves that normally cause muscle cells to contract. It has been used successfully to treat a variety of disorders in which there is a spasm of muscles, including anal fissures.
The toxin is injected into the external sphincter, the internal sphincter, and the intersphincteric groove (an indentation just inside the anus that demarcates the dividing line between external and internal sphincters), or into the fissure itself. The dose is varied from 2.5 to 20 units of toxin in two locations (usually on either side of the fissure).
The frequency of healing of fissures with botulinum toxin is almost 38% and is just for 4-6 months . When fissures recur after treatment, they usually heal again with a second injection. The primary side effect of botulinum toxin is the weakness of the sphincters with varying degrees of incontinence (leakage of stool).
All allopathic treatments are temporary and fissures may return with a hard bowel movement. Recurrent fissures often require a change to another form of treatment. When patients are intolerant or unresponsive to non-surgical treatments, surgery becomes necessary.
becomes necessary.
In short – There is no any treatment for Anal Fissure in allopathy.
Surgery for Anal Fissure
The surgical procedure called partial lateral internal sphincterotomy as the technique of choice for the treatment of anal fissures. In this procedure, the internal anal sphincter is cut starting at its distal-most end at the anal verge and extending into the anal canal for a distance equal to that of the fissure. The cut may extend to the dentate line, but no farther.
The sphincter can be divided in a closed (percutaneous) fashion by tunneling under the anoderm or in an open fashion by cutting through the anoderm. The cut is made on the left or right side of the anus, hence the name “partial lateral internal sphincterotomy.” The posterior midline, where the fissure usually is located, is avoided for fear of accentuating the posterior weakness of the muscle surrounding the anal canal. (Additional weakness posteriorly can lead to what is called a keyhole deformity, so-called because the resulting anal canal resembles an old-fashioned skeleton key. This deformity promotes spoilage and leakage of stool).
Many surgeons decline to cut out the fissure itself during lateral sphincterotomy, this reluctance to remove the fissure is not always appropriate, and the characteristics of the fissure itself should be taken into account. If the fissure is hard and irregular, suggesting anal cancer, the fissure should be biopsied. If the edges and base of the fissure are heavily scarred, there may be a problem after surgery with anal stenosis, a condition in which additional scarring narrows the anal canal and interferes with the passage of stool. In this case, it may be better to cut out the scarred fissure so that there is a chance for the wound to heal with less scarring and the chance of stenosis. Finally, an associated large anal papilla or a large hemorrhoidal tag may interfere physically with wound healing, and removing them may promote healing.
Following surgery, only 53% to 67% of fissures heal. Recurrence rates after this type of surgery are more than, 40%.
Failure to heal following surgery often is attributed to reluctance on the part of the surgeon to adequately divide the internal anal sphincter; other reasons for failure to heal, such as Ulcerative Colitis and/or Crohn’s disease should be considered as well. The risk of incontinence (leakage) of stool following surgery is always there. It is important to distinguish between short-term and long-term incontinence. In the short term (under six weeks), the sphincter is weakened by the surgery, so leakage of stool is not unexpected. Long-term incontinence should not occur after partial lateral internal sphincterotomy because the internal sphincter is less important than the external sphincter (which is not cut) in controlling the passage of stool.
It is important to distinguish between incontinence to gas, a minimal amount of stool that, at most, stains the underwear (soiling), and loss of stool that requires an immediate change in underwear. In a large series of patients followed for a mean of five years after surgery, 26% were incontinent of gas, 38% had minor soiling, and 10% experienced the loss of stool.
Anal surgical stretch for Anal Fissure
Several surgeons have described procedures that stretch and tear the anal sphincters for the treatment of anal fissures. Though anal stretching often is successful in alleviating pain and healing the fissure, it is a traumatic, uncontrolled disruption of the sphincter. Ultrasonography of the anal sphincters following stretching demonstrate trauma that extends beyond the desired area. Because only 72% of fissures heal and there is a 20% incidence of incontinence of stool, stretching has fallen out of favor.
Homeopathic Treatment for Anal Fissure
Treating anal fissure with Homeopathy is very simple, short term and cure is almost for lifetime not temporary. Homeopathy treats not only the fissure itself but it’s cause(s) too.
There lot of medicines for anal fissure and their causes in Homeopathy; Here I (Dr Qaisar Ahmed MD, DHMS) will explain very few of them:
Botulinum:
Toxin of Bacillus Botulinum is best choice for anal sphincter diseases. Weakness of rectal muscles. Ractal stitching pains, burning. Difficulty in passing stool – due to cramping pain and burning. Severe constipation. Rectal muscles weakness. Bulbar paresis.
Aloe Socotrina:
Constant bearing down in rectum; bleeding, sore, and hot; relieved by cold water. Feeling of weakness and loss of power of anal sphincter. Sense of insecurity in rectum, when passing flatus. Uncertain whether gas or stool will come. Stool passes without effort, almost unnoticed. Lumpy, watery stool. Jelly-like stools, with soreness in rectum after stool. A lot of mucus, with pain in rectum after stool. Haemorrhoids protrude like grapes. Anal fissure – very sore and tender; better cold water application. Burning in anus and rectum. Constipation, with heavy pressure in lower part of abdomen.
Thuja Occidentalis
Distended; indurations in abdomen. Chronic diarrhoea, worse after breakfast. Discharges forcibly expelled; gurgling sound. Brown spots. Flatulence and distension; protruding here and there. Rumbling and colic. Constipation, with violent rectal pain, causing stool to recede. Piles swollen; pain worse sitting, with stitching, burning pains at the anus. Anus fissured; painful to touch with warts.
Graphites:
Constipation; large, difficult, knotty stools united by mucus threads. Burning haemorrhoids. Prolapse, diarrhoea; stools of brown fluid, mixed with undigested substance, very fetid, sour odor. Smarting, sore anus, itching. Lump stool, conjoined with threads of mucus. Varices of the rectum. Fissure of anus.
Muriatic Acid:
Tendency to involuntary evacuations while urinating. Haemorrhoids or fissure most sensitive to all touch; even toilet paper is painful. Anal itching and prolapsus while urinating. Haemorrhoids during pregnancy; bluish, hot with violent stitches.
Nitricum Acidum:
Great straining, but little stool passes. Rectum feels torn. Constipated, with anal fissures. Tearing pains during stools. Violent cutting pains after stools, lasting for hours. Haemorrhages from bowels, profuse, bright. Prolapsus ani. Rectum bleed easily. Diarrhoea, slimy and offensive. After stools, irritable and exhausted. Colic relieved from tightening clothes. Jaundice, aching in liver.
fissures. Tearing pains during stools. Violent cutting pains after stools, lasting for hours. Haemorrhages from bowels, profuse, bright. Prolapsus ani. Rectum bleed easily. Diarrhoea, slimy and offensive. After stools, irritable and exhausted. Colic relieved from tightening clothes. Jaundice, aching in liver.
Ratanhia Peruviana:
Aches, as if full of broken glass. Anus aches and burns for hours after stool. Feels constricted. Dry heat at anus, with sudden knife-like stitches. Stools must be forced with great effort; protrusion of haemorrhoids. Fissures of anus, with great constriction, burning; temporarily relieved by cold water. Fetid, thin diarrhoea; stools burn; burning pains before and after stools. Oozing at anus. Itching of anus.
Collinsonia Canadensis:
Pure mucous stools, or mucous stools mixed with dark substances; before stool, severe pain in lower abdomen; during stool, tenesmus; vomiting. Dysenteric stools. Haemorrhoidal dysentery with tenesmus. Obstinate constipation with haemorrhoids and/or anal fissure; stools very sluggish and hard, accompanied by pain and flatulence. Bowels not moved for days, constant pressure in rectum with a heavy dragging ache in pelvis. Piles with constipation, anal fissure, sometimes with diarrhoea, bleeding or blind and protruding. Feeling of sticks, or gravel, or sand in rectum. Itching or burning in anus with swelling.
Aesculus Hippocastanum:
Rectum dry, aching. Feels full of small sticks. Anus raw, sore. Much pain after stool, with prolapse. Haemorrhoids, with sharp shooting pains up the back; blind and bleeding; worse during climacteric. Large, hard, dry stools. Mucous membrane seems swollen and obstructs the passage. Irritation caused by ascarides and aids their expulsion. Burning in anus with chills up and down back.
Sepia Succus/Officianalis:
Bleeding at stool and fullness of rectum. Constipation; large, hard stools; feeling of a ball in rectum, cannot strain; with great tenesmus and pains shooting upward. Dark-brown, round balls glued together with mucus. Soft stool, difficult. Prolapsus ani. Almost constant oozing from anus. Infantile diarrhoea, worse from boiled milk, and rapid exhaustion. Pains shoot up in rectum and vagina. Anal fissure.
Kalium Carbonicum:
Large difficult stools, with stitching pain before and after stool. Haemorrhoids large, swollen, painful, burning. Itching, ulcerated pimples around anus. Large discharge of blood with natural stool. Anal fissure. Pain in haemorrhoids when coughing. Burning in rectum and anus. Easy prolapsus. Itching.
Graphites
Constipation; large, difficult, knotty stools united by mucus threads. Burning

haemorrhoids. Prolapse, diarrhoea; stools of brown fluid, mixed with undigested substance, very fetid, sour odor. Smarting, sore anus, itching. Lump stool, conjoined with threads of mucus. Varices of the rectum. Fissure of anus.
Podophyllum
Diarrhoea of long standing, with hot, glowing cheeks while being bathed or washed; in hot weather after citrus fruits. Morning, painless diarrhoea when not due to venous stasis or intestinal ulceration. Green, watery, fetid, profuse, gushing. Prolapse of rectum before or with stool. Constipation; clay-colored, hard, dry, difficult. Constipation alternating with diarrhoea. Internal and external piles. Anal fissure.
Silicea Terra:
Feels paralyzed. Fistula in ano. Fissures and haemorrhoids, painful, with spasm of sphincter. Stool comes down with difficulty; when partly expelled, recedes again. Great straining; rectum stings; closes upon stool. Feces remain a long time in rectum. Constipation with irritable anal sphincter. Diarrhoea of cadaverous odor.
Berberus Vulgaris
Constant urging to stool. Diarrhoea painless, clay-colored, burning, and smarting in anus and perineum. Tearing around anus. Anal fistulas. Anal fissure.
Sedum Acre:
Painful piles that worse after a few hours of passing stool, pain is constricting. Anal fissure with pain that worsens a few hours after passing stool.
Mercuris Corrosive:
Dysentery; tenesmus, not relieved by stool; incessant. Stool hot, bloody, slimy, offensive, with cutting pains and shreds of mucous membrane.
Mercurius Cyanatus
Intolerable pain. Redness around anus. Fissure. Frequent haemorrhage; stools with tenesmus. Discharge of fetid liquid with gangrenous odor. Black stools.
Mercurius Dulcis
Scanty, bloody mucus, with bile, and constant desire, without tenesmus. Dark-green, watery, with griping. Anus sore and burning. Fissure. Dysentery; small stools of mucus and blood, covered with bile.
Baryta Carbonicum:
Hard and tense, distended. Colicky. Enlarged mesenteric glands. Pain in abdomen swallowing food. Habitual colic, with hunger, but food is refused. Constipation, with hard, knotty stools. Anal fissure. Haemorrhoids protrude on urinating. Crawling in rectum. Oozing at anus.
Lachesis Mutus:
Constipated, offensive stool. Anus feels tight, as if nothing could go through it. Pain darting up the rectum with sneezes or coughs. Rectal fissure. Haemorrhage from bowels like charred straw, black particles. Haemorrhoids protrude, become constricted, purplish. Stitches in them on sneezing or coughing. Constant urging in rectum, not for stool.
Nux vomica:
Blind piles with pronounced burning and itching around the anus. Constant desire to pass stools. Constipation, with frequent ineffectual urging, incomplete and unsatisfactory; feeling as if part remained unexpelled. Rectal constriction. Irregular, peristaltic action; hence frequent ineffectual desire, or passing but small quantities at each attempt. Itching, blind haemorrhoids, with ineffectual urging to stool; very painful; after drastic drugs. Anal fissure. Frequent small evacuations. Scanty stool, with much urging. Dysentery; stools relieve pains for a time. Constant uneasiness in rectum.
Phosphorus:
Very fetid stools and flatus. Long, narrow, hard – difficult to expel. Desire for stool on lying on, left side. Painless, copious debilitating diarrhoea. Green mucus with grains like sago. Involuntary; seems as if anus remained open. Great weakness after stool. Rectal fissure. rectal burning and stinging pains. Discharge of blood from rectum, during stool. White, hard stools. Bleeding haemorrhoids.
Causticum:
Soft and small, size of goose-quill. Hard, tough, covered with mucus; shines like grease; small-shaped; expelled with much straining, or only on standing up. Pruritus. Partial paralysis of rectum. Rectum sore and burns. Fistula and large piles.
Pulsatilla:
Rumbling, watery stools; worse, night No two stools alike. After fruit. Blind haemorrhoids, with itching and sticking pains. Fissure. Dysentery; mucus and blood, with chilliness. Two or three normal stools daily.
Sulphur:
Itching, burning, oozing haemorrhoids accompanied by a feeling of fullness and pressure in the abdomen. The anus is inflamed and red and may protrude significantly. Itching and burning of anus; piles dependent upon abdominal plethora. Frequent, unsuccessful desire; hard, knotty, insufficient. Anal fissure. Redness around the anus, with itching. Morning diarrhoea, painless, drives out of bed, with prolapsus recti. Haemorrhoids, oozing and belching.
Alumina
A very general condition corresponding to this medicine is dryness of mucous membranes and skin, and tendency to paretic muscular states. Stool hard dry, knotty; no desire. Rectum sore, dry, inflamed, bleeding. Itching and burning at anus. Even a soft stool is passed with difficulty. Great straining. Rectal wounds, fissure.
Paeonia Officinalis
Biting, itching in anus; orifice swollen. Burning in anus after stool; then internal chilliness. Fistula ani, diarrhoea, with anal burning and internal chilliness. Painful ulcer, oozing offensive moisture on perineum, anal fissure. Haemorrhoids, fissures, ulceration of anus and perineum, purple, covered with crusts. Atrocious pains with and after each stool. Sudden, pasty diarrhoea, with faintness in abdomen.. Biting, itching in anus; orifice swollen. Burning in anus after stool; then internal chilliness. Fistula ani, diarrhoea, with anal burning and internal chilliness. Painful ulcer, oozing offensive moisture on perineum. Atrocious pains with and after each stool. Sudden, pasty diarrhoea, with faintness in abdomen.
Arnica montana:
Straining of tenesmus in diarrhoea. Offensive, brown, bloody, putrid, involuntary. Looks like brown yeast. Must lie down after every stool. Diarrhoea of consumption; worse lying on left side. Dysenteric stools with muscular pains. Anal fissure. Fistula.
Calcarea Fluorica:
Haemorrhoids with bleeding and itching in the anal region, or internal haemorrhoids causing soreness in the very low back and sacrum. Diarrhoea in gouty subjects. Itching of anus. Fissure of the anus, and intensely sore crack near the lower end of the bowel. Bleeding haemorrhoids. Itching of anus as from pinworms. Internal or blind piles frequently, with pain in back, generally far down on the sacrum, and constipation. Much wind in lower bowels. Worse, pregnancy.
Hamamelis virginiana:
Improves venous circulation and relieves haemorrhoids that are painful with the slightest contact and bleed easily. Anus feels sore and raw. Haemorrhoids, bleeding profusely, with soreness. Dysentery. Pulsation in rectum. Fistula. Anal fissure.
Ignatia:
Haemorrhoids are accompanied by spasms and stabbing pain in the rectum. Stitching pains when coughing. Bleeding and pain are often worse when the stool is loose, and rectal prolapse sometimes follows bowel movements. Itching and stitching in rectum. Prolapse. Stools pass with difficulty; painful constriction of anus after stool. Anal fissure. Diarrhoea from fright. Stitches from anus deep into rectum. Haemorrhage and pain; worse when stool is loose. Pressure as of a sharp instrument from within outward.
Lycopodium Clavatum:
Rectal prolapse. Piles swollen and painful, and the pain gets worse upon touching and sitting. Anal fissure. Chronic constipation with a scanty stool, painful constriction at the anus and excessive flatulence and bloating in the abdomen may also be present.
For consultation; Feel free to whatsapp us or visit our clinic.
P. S : This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
Location, address and contact numbers are given below.
NoN of above mentioned medicine(s) is/are the full/complete treatment, but just hints for treatment; every patient has his/her own constitutional medicine.
To order medicine by courier, please send your details at WhatsApp– +923119884588
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at :
https://www.youtube.com/Dr Qaisar Ahmed