
Helicobacter pylori causes stomach infection and is a major cause of gastritis and peptic and duodenum (first part of the small intestine) ulcers. In case of no treatment, Helicobacter pylori infection could be cause of stomach cancer.
Thank you for reading this post, don't forget to subscribe!Helicobacter pylori (H. pylori or, as it is sometimes termed, stomach bacteria) is a spiral-shaped gram-negative bacterium that can cause chronic inflammation of the inner lining of the stomach (gastritis) and in the duodenum (first part of the small bowel) in humans. This bacterium also is considered a common cause of ulcers worldwide; as many as 90% of people with ulcers are infected with H. pylori. However, many people have these organisms residing in (colonizing or mucosa-associated) their stomach and upper digestive tract and have few or no symptoms. LPS (lipopolysaccharide) is part of the H. pylori outer membrane and can be toxic when the bacteria die and lyse.
Helicobacter pylori could be transmitted through direct contact with saliva, vomit, and other body fluids of the infected person.
Recent studies have investigated the role of Helicobacter pylori infection in the development of gastric mucosa-associated lymphoid tissue (MALT) lymphoma, approximately 0.1% of people infected with Helicobacter pylori develop gastric MALT lymphoma, the role of the CagA antigen, the highest causative agent of Helicobacter pylori, in increasing the risk of gastric MALT lymphoma remains unclear and controversial. A systematic review and meta-analysis were conducted to evaluate the effect of cagA status on the development of gastric MALT lymphoma.
H. pylori multiply in the mucus layer of the stomach lining and duodenum. The bacteria secrete an enzyme called urease that converts urea to ammonia. This ammonia protects the bacteria from stomach acid. As H. pylori multiply, it eats into stomach tissue, which leads to gastritis and/or gastric ulcer.

Symptoms of Helicobacter pylori:
Most individuals with Helicobacter pylori infections have few or no symptoms. Some may experience a few symptoms from mild gastritis episodes, for example,
- Dull or burning pain in stomach (more often a few hours after eating and at night). Pain may last minutes to hours and may come and go over several days to weeks.
- Unplanned weight loss.
- Bloating.
- Nausea and vomiting (bloody vomit).
- Indigestion (dyspepsia).
- Burping.
- Loss of appetite.
- Dark stools (from blood in your stool).
Often, these symptoms simply go away. However, those individuals who have more serious infection experience signs and symptoms of stomach and duodenal ulcers or severe gastritis which include:
- Abdominal pain and/or discomfort that usually does not wax and wane
- Nausea and vomiting sometimes with blood that is red, or the color is like coffee grounds or like vomitus
- Dark or tar-like stools (black color of feces due to bleeding ulcers)
- Fatigue
- Low red blood cell counts due to bleeding
- The full feeling after consuming a small amount of food
- A decreased appetite that is more constant
Other symptoms may include:
- Diarrhea
- Heartburn
- Bad breath (halitosis)
Persons with symptoms of black, tarry stools, and fatigue should seek immediate medical help or go to an emergency department to be evaluated for intestinal bleeding.
Can H. pylori spread (contagious) from person to person?
Helicobacter pylori are contagious. However, sometimes there is a gray area between the terms contagious and colonized. Contagious usually implies that a disease-causing agent is transferred from person to person, while colonization usually implies an agent that simply populates an organ but does not cause disease, even when transferred from person to person.
The gray area occurs when many people have the agent that causes disease in some of them, but not in many others. Some microbiologists consider such organisms as adapting to their human hosts by slowly changing from infecting humans to colonizing them. Although this is speculation, it seems to fit the ongoing situation with H. pylori. However, others think the bacteria become infecting agents when H. pylori’s genetic makeup is triggered by the surrounding GI environment to produce and release enough toxic chemicals to cause the GI tract to become inflamed.
Diagnose Helicobacter pylori infection
Accurate and simple tests for the detection of H. pylori infection include blood antibody tests, urea breath tests, stool antigen tests, and endoscopic biopsies.
Blood tests
For the presence of antibodies to H. pylori can be performed easily and rapidly. However, blood antibodies can persist for years after the complete eradication of H. pylori with antibiotics. Therefore, blood antibody tests (immunoglobulin G or IgG and/or IgA) may be good for diagnosing infection, but they are not good for determining if medication have successfully eradicated the bacterium.
The urea breath test (UBT)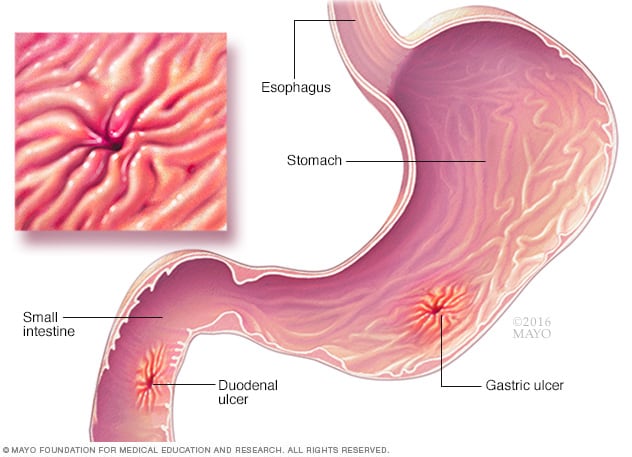
Urea breath is a safe, easy, and accurate test for the presence of H. pylori in the stomach. The breath test relies on the ability of H. pylori to break down the naturally occurring chemical, urea, into carbon dioxide, which is absorbed from the stomach and eliminated from the body in the breath. Ten to 20 minutes after swallowing a capsule containing urea labeled with either a minute amount of radioactive carbon or heavy but not radioactive carbon, a breath sample is collected and analyzed for labeled carbon dioxide. The presence of labeled carbon dioxide in the breath (a positive test) means that there is an active infection. The test becomes negative (there is no radioactive carbon dioxide in the breath) shortly after the eradication of the bacterium from the stomach with allopathic and/or Homeopathic antibiotics. Individuals who are concerned about even minute amounts of radioactivity can be tested with urea labeled with heavy, nonradioactive carbon.
Endoscopy
Endoscopy is an accurate test for diagnosing H. pylori as well as the inflammation and ulcers that it causes. For endoscopy, the doctor inserts an endoscope through the mouth, down the esophagus, and into the stomach and duodenum. During endoscopy, small tissue samples (biopsies) from the stomach lining can be removed and placed on a special slide containing urea (for example, CLO test slides). If the urea is broken down by H. pylori in the biopsy, there is a change in color around the biopsy on the slide. This means that there is an infection with H. pylori in the stomach. Endoscopy also allows the determination of the severity of gastritis with biopsies as well as the presence of ulcers, MALT lymphoma, and cancer.
Biopsies also may be cultured in the bacteriology laboratory for the presence of H. pylori; however, this is done infrequently since other simpler tests are available.
Stool sample
An other test for H. pylori is a test in which the presence of the bacterium can be diagnosed from a sample of stool. The test uses an antibody to H. pylori to determine if H. pylori antigen is present in the stool. If it is, it means that H. pylori are infecting the stomach. Like the urea breath test, in addition to diagnosing infection with H. pylori, the stool test can be used to determine if eradication has been effective soon after treatment.
Allopathic Treatment for Helicobacter pylori
Chronic infection with H. pylori weakens the natural defenses of the lining of the stomach to the ulcerating action of acid. Allopathic drugs that neutralize stomach acid (antacids), and drugs that decrease the secretion of acid in the stomach (H2-blockers and proton pump inhibitors or PPIs) have been used effectively for many years to treat ulcers.
H2-blockers include
- famotidine,
- Omeprazole,
- Cimetidine,
- Ranitidine,
- Nizatidine.

PPIs include
- omeprazole,
- lansoprazole,
- Rabeprazole,
- Pantoprazole,
- Esomeprazole,
- Dexlansoprazole.
Treating H. pylori with acid-reducing antacids, H2-blockers, and PPIs, however, does not eradicate H. pylori from the stomach, and ulcers frequently return promptly after these medications are discontinued. Hence, antacids, H2-blockers, or PPIs have to be taken daily for many years to prevent the return of the ulcers and the complications of ulcers such as bleeding, perforation, and obstruction of the stomach. Even such long-term treatments can fail.
Eradication of H. pylori, however, usually prevents the return of ulcers and ulcer complications even after appropriate medications such as PPIs are stopped. Eradication of H. pylori also is important in the treatment of the rare condition known as MALT lymphoma of the stomach.
Treatment of H. pylori to prevent stomach cancer is controversial and discussed in this article.
Side effects of H2-Blockers
Side effects are usually include diarrhea, constipation, fatigue, drowsiness, headache and muscle aches. The H2 receptor blockers are metabolized in the liver by the cytochrome P450 system.headache, rash, dizziness, and gastrointestinal symptoms including nausea, abdominal pain, flatulence, constipation, and diarrhea. Among the four agents, cimetidine is distinctive in its potent inhibition of the P450 system (CYP 1A2, 2C9 and 2D6), which can result in significant drug interactions. All four H2 receptor blockers have been implicated in rare cases of clinically apparent, acute liver injury.
Cimetidine has been associated with minor elevations in serum aminotransferase levels, Cimetidine is metabolized by and inhibits the function of the microsomal P450 drug metabolizing enzymes, and injury may be the result of its activation to a toxic intermediate. Rapid recurrence with rechallenge is typical. Liver injury have been reported in patients receiving cimetidine, but the time to onset and pattern of injury has varied greatly. Onset can be as short as a few days to as long as 7 months, and the serum enzyme pattern varies from hepatocellular to cholestatic, most cases having a “mixed” hepatocellular-cholestatic pattern of injury (Cases 1 and 2). Liver biopsy histology often shows prominently centrolobular necrosis. Immunoallergic features (rash, fever, eosinophilia) are uncommon, as is autoantibody formation.
Chronic therapy with famotidine has been associated with minor elevations in serum aminotransferase levels. Famotidine is metabolized by the microsomal P450 drug metabolizing enzymes and injury may be the result of its activation to a toxic intermediate, serum enzyme pattern has typically been hepatocellular. Instances of clinically apparent liver injury have been reported in patients receiving famotidine, but few cases have been reported and clinical characteristics in published cases have varied in the time to onset and pattern of injury.
Chronic therapy with nizatidine and other H2 blockers is associated with minor elevations in serum aminotransferase levels. Nizatidine is metabolized by the microsomal P450 drug metabolizing enzymes and injury may be the result of its activation to a toxic intermediate. Instances of clinically apparent liver injury have been reported in patients receiving nizatidine. The typical pattern of serum enzyme elevations varies from hepatocellular to cholestatic, most cases being “mixed”. The injury can be severe, but is typically mild-to- moderate in severity and self-limited in course. Immunoallergic features (rash, fever, eosinophilia) are uncommon, as is autoantibody formation. Liver biopsy histology often shows centrolobular (zone 3) necrosis with mixed cellular infiltrates and mild cholestasis.
Chronic therapy with ranitidine has been associated with minor elevations in serum aminotransferase levels. Ranitidine is metabolized by the microsomal P450 drug metabolizing enzymes and inhibits the function of CYP 3A and 2D6, and injury may be the result of its activation to a toxic intermediate. Rapid recurrence with rechallenge is typical, but features of hypersensitivity are uncommon. Instances of clinically apparent liver injury have been reported in patients receiving ranitidine, but the time to onset and pattern of injury has varied greatly. Onset can be as short as a few days to as long as several months. The pattern of serum enzyme elevation varies from hepatocellular to cholestatic, most cases being “mixed” hepatocellular-cholestatic. The injury is rarely severe and usually resolves rapidly upon stopping, generally within 4 to 12 weeks. Liver biopsy histology often shows prominently centrolobular necrosis. Immunoallergic features (rash, fever, eosinophilia) can occur but are uncommon, as is autoantibody formation.
Side effects of PPI
PPIs are believed to have few adverse effects, as they are generally well tolerated. Patients have experienced few side effects of short-term PPI use, such as headache, rash, dizziness, and gastrointestinal symptoms including nausea, abdominal pain, flatulence, constipation, and diarrhea.
As the use of these drugs increases, reports of their side effects are increasing, particularly with long‐term use. In recent studies, researchers advised that PPIs should be used for the shortest time period at the smallest effective dose, as infections, impaired absorption of nutrients, dementia, kidney disease, and hypergastrinemia-related side effects are emerging as possible consequences of long-term use. Therefore, the aim of this review is to describe the association between PPI use and the risk of serious adverse effects given the increasing concerns about the overuse of PPIs in the general population.
Case reports have linked PPI use with acute kidney injury, chronic kidney disease, patients who used PPIs for longer durations had higher risk of CKD. The main mechanism leading to renal pathology due to PPI use could be acute interstitial nephritis. More than half of the patients who suffered PPI-induced acute interstitial nephritis did not fully recover. PPI-induced CKD is due to progression of acute interstitial nephritis with inflammatory interstitial infiltrates and edema to chronic interstitial scarring and tubular atrophy. Taken together, these findings represent evidence that PPIs cause acute interstitial nephritis and some evidence that they also increase the risk of CKD.
Gastrointestinal Infections
PPI use has been linked with increased risk of both incidental and recurrent Clostridium difficile infections. Acid secretion by parietal cells is an important immunological barrier in the gastrointestinal tract, which is why hypochlorhydria generated by the inhibition of gastric acid secretion increases the risk of bacterial colonization and altered intestinal flora and susceptibility to enteric infections. Studies have demonstrated that intense suppression of gastric acid secretion is associated with increased risk of Clostridium difficile infection. Authors reported that more than two-thirds of inpatient acid-suppressive prescriptions are not strictly indicated and the number of Clostridium difficile infection cases are in the millions per year.
Authors have reported other enteric infections, such as non-typhoid Salmonella and Campylobacter infections, the latter of which has been racing.
Respiratory Infections
Pneumonia has been widely associated with PPI use, especially over the short term (usually fewer than 30-90 days). The most likely explanation for the increased risk of respiratory infections with PPI use is that PPI-induced hypochlorhydria increases microaspiration of gastric contents, which increases lung colonization and the subsequent incidence of pneumonia.
PPI use also maybe associated with an increased risk of coronavirus disease 2019 (COVID-19), as authors have reported that patients using PPI drugs had higher odds of testing positive for COVID-19 than did patients not taking PPIs.
Coronaviruses are easily destroyed by an acidic gastric pH, although the impact of acid suppression is unclear. Previously reported data suggested that the infectivity of severe acute respiratory syndrome coronavirus 1 was reduced in individuals with a gastric pH of up to 3. Furthermore, researchers have shown coronaviruses to survive in individuals with more basic gastric pH levels, including those in the range created by the use of drugs like omeprazole and esomeprazole. Current and past PPI use were associated with poor outcomes of COVID-19. Receptors for COVID-19 (ACE-2) are found throughout the gastrointestinal tract, making plausible the hypothesis that PPI users may be more vulnerable than nonusers to the effect of high viral loads.
Gastrointestinal malignancies
Because PPIs decrease gastric acid secretion, compensatory raising of gastrin levels in patients has a proliferative effect on the growth of enterochromaffin-like cells, explaining the association of PPIs with development of neuroendocrine tumors and carcinomas of the gastrointestinal tract. Another related mechanism is that PPIs facilitate gastric pan-colonization by Helicobacter pylori due to a decrease in the normal stomach acidic environment. Numerous mechanistic studies suggested that hypoacidity and hypergastrinemia increase the risk of gastric cancer in the corpus/fundus, which was supported by epidemiological studies.
Liver disease
PPI use has been linked with increased risk of cirrhosis-related complications such as hepatic encephalopathy, spontaneous bacterial peritonitis, and liver cancer. These effects appear to be related to chronic PPI use, as patients who underwent more than six months of follow-up after initiating treatment with PPIs had twice the risk of hepatocellular carcinoma. The mechanism of liver injury associated with PPI use, is not completely understood, although investigators observed that H+/K+ ATPase inhibition leads to intestinal bacterial overgrowth and an altered intestinal microbial composition, which may lead to increased portal venous concentrations of several potentially harmful substances, including secondary bile acids. PPIs are metabolized in the liver; therefore, patients with liver disease may be at risk for increased hepatotoxicity, which can lead to hypergastrinemia-induced carcinogenic effects, especially on liver cells. Finally, the authors reported that after exposure to PPIs, cultured human liver cells exhibited gene expression similar to well-known carcinogens in the liver.
Fracture risk
Increased fracture risk due to PPI intake is a conferemed study. Retrospective studies have suggested the existence of a dose-dependent relationship between PPIs and decreased bone mineral density, leading to an increase in fracture risk, especially hip fractures.
The risk appears to be higher in patients with a risk factor for osteoporosis, such as renal dysfunction. Routine prophylaxis for osteoporosis is suggested for PPI users to prevent osteoporotic fractures. Proposed mechanisms that link PPI-based therapy with decreased bone mineral density include hypochlorhydria-associated malabsorption of calcium (absorption of which is indispensable to maintaining bone microstructure), gastrin-induced parathyroid hyperplasia, and inhibition of bone resorption by blocking local H+/K+ ATPase.
Dementia
Overall, data on the association between PPI use and dementia risk is very wide. With uncertainty about the mechanism, most cases of brain dysfunction in PPI users are reported to be associated with chronic administration of PPIs. Some PPIs, such as lansoprazole, esomeprazole, and pantoprazole, have been linked with neurological side effects, such as headaches and dizziness/vertigo, central nervous system include depression, diplopia, disturbed sleep, drowsiness, insomnia, nervousness, tremor, sensory and perceptual abnormalities (e.g., hallucinations), and delirium.
Although the mechanisms are not completely understood, the neurological effects of PPIs appear to be explained by the influence in ionic pumps controlling the membrane potential in neurons. The lysosomes of patients taking PPIs seem to be less acidic than those of patients not taking them, which may make cells less able to degrade amyloid-beta protein, the principal substance that accumulates in the brain in patients with Alzheimer’s disease. Other hypotheses include that PPI and H2 receptor antagonist use have indirect effects related to systemic abnormalities (i.e., magnesium and vitamin B12 deficiency).
Cardiovascular disease
Over the past decade, PPI use has been associated with cardiovascular morbidity and mortality. Increased risk of major acute cardiovascular events, including acute myocardial infarction and stroke, has been correlated with lengthy or high-dose treatment with PPIs. Also, there is a concern that theoretical risk of malignant ventricular arrhythmias has been warned due to the development of hypomagnesemia, which may lengthen the QT interval and lead to torsade de pointes. PPI use may lead to reduction of endothelial nitrous oxide levels through inhibition of dimethylarginine dimethylaminohydrolase enzymatic activity, which is responsible for clearance of asymmetric dimethylarginine, thereby reducing nitrous oxide synthase activity. PPIs seem to increase the blood levels of chromogranin A, an important marker of neuroendocrine tumors that investigators have also proposed to be a biomarker of cardiovascular disease. Chromogranin A and its derived peptides, vaso statins and catestatin, elicit vasodilatory and cardioregulatory effects that may be adaptive over the short term and maladaptive over the long term. Finally, PPIs impair clopidogrel antiplatelet effect due to competition for the cytochrome P450 isoenzyme CYP2C19.
Other, less prevalent side effects of PPIs are myopathy, hypomagnesemia, anemia, fundic gland polyps, micronutrient deficiencies, and subacute cutaneous lupus erythematosus
Allopathic treatment for Helicobacter pylori 
allopathically H. pylori are difficult to eradicate/cure from the stomach because it is capable of developing resistance to commonly used allopathic antibiotics (antibiotic-resistant H. pylori). Therefore, two or more antibiotics usually are given together with a PPI and/or bismuth-containing compounds to eradicate the bacterium. (Bismuth and PPIs have anti-H. pylori effects.) Examples of combinations of medications that are effective are:
- a PPI, amoxicillin (Amoxil), and clarithromycin
- a PPI, metronidazole (Flagyl), tetracycline, and bismuth subsalicylate (Pepto-Bismol, Bismuth)
These combinations of medications can be expected to cure 70% to 90% of infections. However, studies have shown that resistance of H. pylori (failure of antibiotics to eradicate the bacterium) to clarithromycin is common among patients who have prior exposure to clarithromycin or other chemically similar macrolide antibiotics (such as erythromycin).
Similarly, H. pylori resistance to metronidazole is common among patients who have had prior exposure to metronidazole. In these patients, doctors have to find other combinations of antibiotics to treat H. pylori. Antibiotic resistance is another reason why antibiotics should be used carefully and judiciously for the right reasons, and indiscriminate use of antibiotics for improper reasons should be discouraged.
First-line regimens for Helicobacter pylori eradication or cure are taken from the guidelines developed by the American College of Gastroenterology as follows:
- Standard dose of a *PPI (proton pump inhibitor) *b.i.d. (esomeprazole is *q.d.),clarithromycin 500 mg b.i.d., amoxicillin 1,000 mg b.i.d. for 10-14 days
- Standard dose PPI b.i.d., clarithromycin 500 mg b.i.d. metronidazole 500 mg b.i.d. for 10-14 days
- Bismuth subsalicylate 525 mg p.o. q.i.d. metronidazole 250 mg * p.o. *q.i.d., tetracycline 500 mg p.o. q.i.d., ranitidine 150 mg p.o. b.i.d. or standard dose PPI q.d. to b.i.d. for 10-14 days
- PPI + amoxicillin 1 g b.i.d., for 5 days, followed by PPI, clarithromycin 500 mg, tinidazole 500 mg b.i.d. for 5 days (used mainly in other countries)
*PPI = proton pump inhibitor; pcn = penicillin; p.o. = orally; q.d. = daily; b.i.d. = twice daily; t.i.d. = three times daily; q.i.d. = four times daily.
Triple therapy of either levofloxacin or rifabutin in combination with amoxicillin and esomeprazole yielded cure rates of 90% and 88.6%. (levofloxacin 20=50 mg b.i.d. or rifabutin 150 mg q.d. Amoxicillin dose 1 gm, esomeprazole 40 mg, both b.i.d.).
Some doctors may want to confirm eradication of H. pylori after treatment with a urea breath test or a stool antigen test, particularly if there have been serious complications of the infection such as perforation or bleeding in the stomach or duodenum. Endoscopic biopsies to determine eradication of the bacterium are not necessary, and blood tests are not good for determining eradication since it takes many months or years for the antibodies to H. pylori to decrease. Patients who fail to eradicate H. pylori with treatment are retreated, often with a different combination of medications. Also, a meta-analysis study of patients started on low-dose aspirin showed less than 20% were tested for H. pylori; this is concerning because low-dose aspirin roughly doubles the risk factors for getting an upper GI bleed in individuals with H. pylori infection.
Homeopathic treatment for Helicobacter pylori 
Homeopathic treatment for H. pylori is very effective, short term and without any side effects. Few Homeopathic medicines for H. pylori are:
Bismuthum Metallicum
Nausea after every meal. Water is vomited as soon as it reaches the stomach, vomiting of brownish matter, of bile. Nausea, with inclination to vomit. Violent risings of a putrid smell. Cancer of stomach. Cramp-like and precisive pains in the stomach. Burning in the stomach. Inflammation of the stomach. Borborygmi and rumbling in the abdomen. Colic with pinching, pressure, and an inclination to go to stool. Great inflation of the abdomen. Abdomen bloated in ridges; rumbling of wind along colon, passes rarely, but then relieves. Painful sensibility of the abdomen to the touch.
Inflammation of the whole throat. Burning pain in the throat, sometimes insupportable. Phagedenic ulceration of uvula, with burning and tearing; difficult swallowing of fluids, which return through nose.
Ineffectual efforts to go to stool. Aqueous diarrhoea of a putrid smell. Stools are cadaverous smell. Cholera; cholerine; fluids vomit as soon as taken.
Nux Vomica
Sour taste, and nausea in the morning, after eating. Weight and pain in stomach; worse, eating, some time after. Flatulence and pyrosis. Sour, bitter eructation. Nausea and vomiting, with much retching. Ravenous hunger, especially about a day before an attack of dyspepsia. Region of stomach very sensitive to pressure. Epigastrium bloated, with pressure like a stone, several hours after eating. Desire for stimulants. Loves fats and tolerates them well (Puls opposite). Dyspepsia from drinking strong coffee. Difficult belching of gas. Wants to vomit, but cannot.
Abdomen : Bruised soreness of abdominal walls. Flatulent distension, with spasmodic colic. Colic from uncovering. Liver engorged, with stitches and soreness. Colic, with upward pressure, causing short breath, and desire for stool. Weakness of abdominal ring region. Strangulated hernia. Forcing in lower abdomen towards genitals. Umbilical hernia of infants.
Constipation, with frequent ineffectual urging, incomplete and unsatisfactory; feeling as if part remained unexpelled. Constriction of rectum. Irregular, peristaltic action; hence frequent ineffectual desire, or passing but small quantities at each attempt. Absence of all desire for defecation is a contra-indication. Alternate constipation and diarrheas – after abuse of purgatives. Urging to stool felt throughout abdomen. Itching, blind hemorrhoids, with ineffectual urging to stool; very painful; after drastic drugs. Diarrheas after a debauch; worse, morning. Frequent small evacuations. Scanty stool, with much urging. Dysentery; stools relieve pains for a time. Constant uneasiness in rectum. Diarrheas, with jaundice.
Bryonia Alba
Nausea and faintness in morning. Abnormal hunger, loss of taste. Thirst for large draughts. Vomiting of bile and water immediately after eating. Worse, warm drinks, which are vomited. Stomach sensitive to touch. Pressure in stomach after eating, as of a stone. Soreness in stomach when coughing. Dyspeptic ailments during summer heat. Sensitiveness of epigastrium to touch.
Liver region swollen, sore, tensive. Burning pain, stitches; worse, pressure, coughing, breathing. Tenderness of abdominal walls.
Constipation; stools hard, dry, as if burnt; seem too large. Stools brown, thick, bloody; worse in morning, from moving, in hot weather, after being heated, from cold drinks, every spell of hot weather.
Apis Mellifica
Sore feeling. Thirstless. Vomiting of food. Abdomen sore, bruised on pressure, when sneezing. Extremely tender. Dropsy of abdomen. Peritonitis. Swelling in right groin. Stool involuntary on every motion; anus seems open. Bloody, painless. Anus feels raw. Haemorrhoids, with stinging pain, after confinement. Diarrhoea watery, yellow; cholera infantum type. Cannot urinate without a stool. Dark, fetid, worse after eating. Constipation; feels as if something would break on straining.
Natrum Muriaticum
Frothy coating on tongue, with bubbles on side. Sense of dryness. Scorbutic gums. Numbness, tingling of tongue, lips, and nose. Vesicles and burning on tongue, as if there was a hair on it. Eruptions around mouth and vesicles like pearls on lips. Lips and corners of mouth dry, ulcerated, and cracked. Deep crack in middle of lower lip. Tongue mapped. Loss of taste. Large vesicle on lower lip, which is swollen and burns. Immoderate thirst.
Hungry, yet loose flesh. Heartburn, with palpitation. Unquenchable thirst. Sweats while eating. Craving for salt. Aversion to bread, to anything slimy, like oysters, fats. Throbbing in pit. Sticking sensation in cardiac orifice. Cutting pain in abdomen. Distended. Pain in abdominal ring on coughing.
Rectum burning, pains and stitching after stool. Anus contracted, torn, bleeding. Constipation; stool dry, crumbling. Painless and copious diarrhoea, preceded by pinching pain in abdomen.
Ammonium Muriaticum
Thirst for lemonade, regurgitation of food (gastrointestinal reflux disease {GERD}), bitter water brash. Nausea. Gnawing in stomach. Epigastric pain immediately after eating. Cancer of stomach. Splenic stitches, especially in the morning, with difficult breathing. Pain around navel. Abdominal symptoms appear during pregnancy. Chronic congestion of liver. Excessive fatty deposit around abdomen. Much flatus. Strained feeling in groin.
Rectum itching and haemorrhoids, soreness with pustules. Hard, crumbly stool, or covered with glairy mucus. Stinging in perineum. Green mucus stools alternate with constipation. During and after stool, burning and smarting in rectum. Haemorrhoids after suppressed leucorrhoea.
Magnesium Muriaticum
Blisters on lips. Gums swollen, bleed easily. Tongue feels burnt and scalded. Throat dry, with hoarseness. Appetite poor, had taste in mouth. Eructations like rotten eggs. Continued rising of while froth into mouth Cannot digest milk. Urine can be passed only by pressing abdominal muscles. Pressing pain in liver; worse lying on right side. Liver enlarged with bloating of abdomen; yellow tongue. Congenital scrotal hernia. Must use abdominal muscles to enable him to urinate.
Constipation during dentition; Adult – only passing small quantity; stools knotty, like sheep’s dung, crumbling at verge of anus. Painful smarting haemorrhoids.
Taraxacum Officinale
Gastric headaches, bilious attacks, with characteristically mapped tongue and jaundiced skin. Cancer of bladder. Flatulence. Hysterical tympanites. Sensation of great heat on top of head. Sternomastoid muscle very painful to touch. Mapped tongue. Tongue covered with a white film; feels raw; comes off in patches, leaving red, sensitive spots. Loss of appetite. Bitter taste and eructations. Salivation.
Liver enlarged and indurated. Sharp stitches in left side. Sensation of bubbles bursting in bowels. Tympanites. Evacuation difficult.
Rhus Toxicodendron
Want of appetite for any kind of food, with unquenchable thirst. Bitter taste. Nausea, vertigo, and bloated abdomen after eating. Desire for milk. Great thirst, with dry mouth and throat. Pressure as from a stone. Drowsy after eating.
Violent abdominal pains, relieved by lying on abdomen. Swelling of inguinal glands. Pain in region of ascending colon. Colic, compelling to walk bent. Excessive distention after eating. Rumbling of flatus on first rising, but disappears with continued motion.
Diarrhoea of blood, slime, and reddish mucus. Dysentery, with tearing pains down thighs. Stools of cadaverous odor. Frothy, painless stools. Will often abort a beginning suppurative process near the rectum. Dysentery.
Sulphur
Complete loss of, or excessive appetite. Putrid eructation. Food tastes too salty. Drinks much, eats little. Milk disagrees. Great desire for sweets. Great acidity, sour eructation. Burning, painful, weight-like pressure. Very weak and faint about 11 am; must have something to eat. Nausea during gestation. Water fills the patient up.
Abdomen very sensitive to pressure; internal feeling of rawness and soreness. Movements as of something alive. Pain and soreness over liver. Colic after drinking.
Rectum itching and burning of anus; piles dependent upon abdominal plethora. Frequent, unsuccessful desire; hard, knotty, insufficient. Child afraid on account of pain. Redness around the anus, with itching. Morning diarrhoea, painless, drives out of bed, with prolapsus recti. Haemorrhoids, oozing and belching.
Digitalis Purpurea
Sweet taste with constant ptyalism. Excessive nausea, not relieved by vomiting. Faintness, great weakness in stomach. Burning in stomach extending to oesophagus. Faintness and vomiting from motion. Discomfort, even after a small quantity of food, or from mere sight or smell. Tenderness of epigastrium. Copious salivation. Neuralgic pain in stomach, unconnected with taking food.
Pain in left side of abdomen apparently in descending colon and under false ribs. Severe abdominal pains, pulsation in abdominal aorta, and epigastric constriction. Enlarged, sore, painful liver. Stool white, chalk-like, ashy, pasty stools. Diarrhoea during jaundice.
Colocynth
The colocynth stomach pains are clutching, cramping and digging, as if grasped by the fingers. Similar pains occur lower down in the abdomen, but they are still better from hard pressure, and from doubling up which amounts to pressure come on in paroxysms of increasing severity, until the patient is nauseated and vomits, and are associated with great restlessness and faint, sinking feeling at the pit of the stomach. The victim bends down over the back of a chair, or over the foot-board, if unable to get out of bed.
Carbo Vegetabilis
Eructation, heaviness, fullness, and sleepiness; tense from flatulence, with pain; worse lying down. Eructation after eating and drinking. Temporary relief from belching. Rancid, sour, or putrid eructation. Waterbrash, asthmatic breathing from flatulence. Nausea in the morning. Burning in stomach, extending to back and along spine. Contractive pain extending to chest, with distention of abdomen. Faint gone feeling in stomach, not relieved by eating. Crampy pains forcing patient to bend double. Distress comes on a half-hour after eating. Sensitiveness of epigastric region. Digestion slow; food putrefies before it digests. Gastralgia of nursing women, with excessive flatulence, sour, rancid belching. Aversion to milk, meat, and fat things. The simplest food distresses. Epigastric region very sensitive.
Abdomen : Pain as from lifting a weight; colic from riding in a carriage; excessive discharge of fetid flatus. Cannot bear tight clothing around waist and abdomen. Ailments accompanying intestinal fistulae. Abdomen greatly distended; better, passing wind. Flatulent colic. Pain in liver.
Rectum and Stool : Flatus hot, moist, offensive. Itching, gnawing and burning in rectum. Acrid, corrosive moisture from rectum. A musty, glutinous moisture exudes. Soreness, itching moisture of perineum at night. Discharge of blood from rectum. Burning at anus, burning varices (Mur ac). Painful diarrheas of old people. Frequent, involuntary cadaverous-smelling stools, followed by burning. White hemorrhoids; excoriation of anus. Bluish, burning piles, pain after stool.
Arsenicum Album
Arsenic Album is a suitable prescription when burning in abdomen is accompanied by marked anxiety.
Nausea, retching, vomiting, after eating or drinking. Anxiety in pit of stomach. Burning pain. Craves acids and coffee. Heartburn; gulping up of acid and bitter substances which seem to excoriate the throat. Long-lasting eructation. Vomiting of blood, bile, green mucus, or brown-black mixed with blood. Stomach extremely irritable; seems raw, as if torn. Gastralgia from slightest food or drink. Dyspepsia from vinegar, acids, ice-cream, ice-water, tobacco. Terrible fear and dyspnea, with gastralgia; also faintness, icy coldness, great exhaustion. Malignant symptoms. Everything swallowed seems to lodge in the esophagus, which seems as if closed and nothing would pass. Ill effects of vegetable diet, melons, and watery fruits generally. Craves milk.
Abdomen : Gnawing, burning pains like coals of fire; relieved by heat. Liver and spleen enlarged and painful. Ascites and anasarca. Abdomen swollen and painful. Pain as from a wound in abdomen on coughing.
Rectum : Painful, spasmodic protrusion of rectum. Tenesmus. Burning pain and pressure in rectum and anus.
Stool : Small, offensive, dark, with much prostration. Worse at night, and after eating and drinking; from chilling stomach, alcoholic abuse, spoiled meat. Dysentery dark, bloody, very offensive. Cholera, with intense agony, prostration, and burning thirst. Body cold as ice. Hemorrhoids burn like fire; relieved by heat. Skin excoriated about anus.
Ipecacuanha
Ipecac should be prescribed when there is nausea – all the time. Vomiting of white glairy mucus or food appears, but the nausea is not relieved even after vomiting. Mouth, moist; much saliva. Constant nausea and vomiting. Vomits food, bile, blood, mucus. Stomach feels relaxed, as if hanging down. Hiccough.
Amebic dysentery with tenesmus; while straining pain so great that it nauseates; little thirst. Cutting, clutching; worse, around the navel. Body rigid; stretched out stiff. Stools Pitch-like green as grass, like frothy molasses, with griping at navel. Dysenteric, slimy.
Antimonium Crudum
Antimonium Crudum should be advised when belching is constant. Belching in such cases tastes mainly of eaten food. Dyspepsia and vomiting may also be present. Eructation tasting of the ingesta. Heartburn, nausea, vomiting. After nursing, the child vomits its milk in curds, and refuses to nurse afterwards, and is very cross. Gastric and intestinal complaints from bread and pastry, acids, sour wine, cold bathing, overheating, hot weather. Gouty metastasis to stomach and bowels. Sweetish water brash. Bloating after eating.
Diarrhea alternating with constipation, especially in old people. Diarrhea after acids/acidic food and/or drinks, after baths, overeating; slimy, flatulent stools. Mucous piles, continued oozing of mucus. Hard lumps mixed with watery discharge. Catarrhal proctitis. Stools composed entirely of mucus.
Phosphorus
Phosphorus should be advised when there is marked pain and burning in the stomach/epigastrium relieved by cold food/drinks, ice. The pain gets worse from even touching and walking. The burning extends to the throat and intestines. Cold food relieves gastric complaints. Sour taste and sour eructation after every meal.
Belching large quantities of wind, after eating. Throws up ingesta by the mouthfuls. Vomiting; water is thrown up as soon as it gets warm in the stomach. Postoperative vomiting. Throat opening feels contracted, too narrow; the food scarcely swallowed, comes up again.
Argentum Nitricum
Belching accompanies gastritis. Nausea, retching, vomiting of glairy mucus. Flatulence; painful swelling of pit. Painful spot over stomach that radiates to all parts of the abdomen. Gnawing ulcerating pain; burning and constriction. Ineffectual effort at eructation. Great craving for sweets, Desire for cheese and salty food.
Watery, noisy, flatulent; green, like chopped spinach, with shreddy mucus and enormous distention of abdomen; very offensive. Diarrhea immediately after eating or drinking. Fluids go right through; after sweets, After any emotion with flatulence. Itching of anus.
Kali Bichrome
Nausea and vomiting immediately after eating. Feels as if digestion had stopped. Dilatation of stomach. Gastritis. Round ulcer of stomach. Stitches in region of liver and spleen and through to spine. Dislikes water. Cannot digest meat. Desire for beer and acids. Gastric symptoms are relieved after eating, and the rheumatic symptoms reappear (alternate). Vomiting of bright yellow water.
Cutting pain in abdomen, soon after eating. Chronic intestinal ulceration. Soreness in right hypochondrium, fatty infiltration of liver and increase in soft fibrous tissue (cirrhosis). Painful retraction, soreness and burning.
Jelly like stool, gelatinous; worse, mornings. Dysentery; tenesmus, stools brown, frothy. Sensation of a plug in anus. Periodic constipation, with pain across the loins. Brown urine.
Graphites
Nausea and vomiting after each meal. Morning sickness during menstruation. Pressure in stomach, Fullness and hardness in abdomen, as from incarcerated flatulence; must loosen clothing; presses painfully at abdominal ring, constrictive pain in stomach relives temporarily after eating or drink something hot or by lying down.
Croaking in abdomen. Inguinal region sensitive, swollen. Colic pain, Pain of gas opposite the side on which he lies. Chronic diarrhea, stools brownish, liquid, undigested, offensive.
Constipation; large, difficult, knotty stools united by mucus threads. Burning hemorrhoids. Prolapse, diarrheas; stools of brown fluid, mixed with undigested substance, very fetid, sour odor. Smarting, sore anus, itching. Lump stool, conjoined with threads of mucus. Varices of the rectum. Fissure of anus.
Ratanhia
Mawkish taste in morning, in bed. Thirst; in evening. Anorexia, with dislike to food and drink. Constant desire to eat. Risings, with taste of food; empty. Violent hiccough, which causes pain in stomach. Long-continued hiccough after dinner. Nausea and disgust, with retching and vomiting of food. Vomiting of water; of mucus streaked with blood. Pains as from ulceration in stomach. Excessive distension of stomach. Stomach feels too full. Digestion more difficult. Rolling and constriction in stomach. Painful constriction of stomach. Sensation in stomach, and above scrobiculus. Heat and burning sensation in stomach and epigastrium. Sudden painful bursting in pit of stomach.
Repeated violent sticking in hypochondrium. Shootings, pinchings, and contraction of groins. Pinching in both groins. Griping in lower abdomen, externally violent itching. Constrictive pain in small spot in groins; in groin.
13. Stool hard and broken evacuations, with urgent want to evacuate (with straining) and protrusion of haemorrhoidal excrescences. Ineffectual want to evacuate, with pains. Great protrusion of haemorrhoids, with burning in anus. Sudden stitches. Fissures; excruciating pains immediately after stool, if costive. Fissure with constriction. Burning in anus before and during a diarrhoea-like stool. Very urgent desire for normal stool. Diarrhoea with evacuation of some drops of blood. Stool yellow, diarrhoea-like, with burning in anus. Sensation as if splinters of glass sticking in anus and rectum in every direction. Severe itching in anus. Pinworms. Soft loose evacuations, preceded by cuttings, with burning pains in anus, before and after. Thin, fetid stools, burning like fire in anus. Sanguineous diarrhoea. Discharge of blood from the rectum, with or without stool. Pains in head, as if it would burst (during and) after evacuation.
P.S : In treatment of H. pylori always advise potency in 200 & TDs. (Dr. Qaisar Ahmed MD, DHMS, Isl. Jurisprudence).
P. S : This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
Location, address and contact numbers are given below.
NoN of above mentioned medicine(s) is/are the full/complete treatment, but just hints for treatment; every patient has his/her own constitutional medicine.
To order medicine by courier, please send your details at WhatsApp– +923119884588
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS), Abdominal Surgeries, Oncological surgeries, Gastroenterologist, Specialist Homeopathic Medicines.
Senior research officer at Dnepropetrovsk state medical academy Ukraine.
Location: Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr Sayed Qaisar Ahmed at :
https://www.youtube.com/Dr Qaisar Ahmed
https://www.facebook.com/dr.qaisar.dixecosmetics
Comments are closed.