In other words – osteoporosis is a condition characterized by a decrease in the density of bone, decreasing its strength and resulting in fragile bones.
Thank you for reading this post, don't forget to subscribe!Osteoporosis literally leads to the abnormally porous bone that is compressible, like a sponge. This disorder of the skeleton weakens the bone and results in frequent fractures.
Osteopenia, is a condition of bone that is slightly less dense than normal bone but not to the degree of bone in osteoporosis.
Normal bone is composed of protein, collagen, and calcium, all of which give bone its strength. Bones that are affected by osteoporosis can break (fracture) with relatively minor injuries that normally would not cause a bone to fracture.
The fracture can be either in the form of cracking (as in a hip fracture) or collapsing (as in a compression fracture of the vertebrae of the spine). The spine, hips, ribs, and wrists are common areas of bone fractures from osteoporosis although osteoporosis-related fractures can occur in almost any skeletal bone.
What are the consequences of Osteoporosis and Osteopenia
Osteoporotic bone fractures are responsible for considerable pain, decreased quality of life, lost workdays, and disability.
- Up to 30% of patients suffering a hip fractures will require long-term nursing-home care.
- Elderly patients can develop pneumonia and blood clots in the leg veins that can travel to the lungs (pulmonary embolism) due to prolonged bed rest after the hip fracture.
- Osteoporosis has even been linked with an increased risk of death. Some 20% of women with a hip fracture will die in the subsequent year as an indirect result of the fracture.
- In addition, once a person has experienced a spine fracture due to osteoporosis, he or she is at a very high risk of suffering another such fracture in the near future (next few years).
- About 20% of postmenopausal women who experience a vertebral fracture will suffer a new vertebral fracture of a bone in the following year.

22 causes of Osteoporosis and Osteopenia and risk factors
The following are 22 factors that will increase the risk of developing osteoporosis:
- Female gender
- European or cold areas/countries
- Thin and small body frame
- Family history of osteoporosis (for example, having a mother with an osteoporotic hip fracture doubles your risk of hip fracture)
- Personal history of fracture as an adult
- Tobacco smoking
- Alcohol consumption
- Lack of exercise
- Diet low in calcium
- Poor nutrition and poor general health, especially associated with chronic inflammation or bowel disease
- Malabsorption (nutrients are not properly absorbed from the gastrointestinal system) from bowel diseases, such as celiac sprue that can be associated with skin diseases, such as dermatitis herpetiformis.
- Low estrogen levels in women (which may occur in menopause or with early surgical removal of both ovaries).
- Low testosterone levels in men (hypogonadism)
- Chemotherapy can cause early menopause due to its toxic effects on the ovaries
- Amenorrhea (loss of the menstrual period) in young women is associated with low estrogen and osteoporosis; amenorrhea can occur in women who undergo extremely vigorous exercise training and in women with very low body fat (for example, women with anorexia nervosa)
- Chronic inflammation, due to chronic inflammatory arthritis or diseases, such as rheumatoid arthritis or liver diseases.
- Immobility, such as after a stroke, or from any condition that interferes with walking
- Hyperthyroidism is a condition wherein too much thyroid hormone is produced by the thyroid gland (as in Grave’s disease) or is ingested as thyroid hormone medication.
- Hyperparathyroidism is a disease wherein there is excessive parathyroid hormone production by the parathyroid gland, a small gland located near or within the thyroid gland. Normally, the parathyroid hormone maintains blood calcium levels by, in part, removing calcium from the bone. In untreated hyperparathyroidism, the excessive parathyroid hormone causes too much calcium to be removed from the bone, which can lead to osteoporosis.
- When vitamin D is lacking, the body cannot absorb adequate amounts of calcium from the diet to prevent osteoporosis. Vitamin D deficiency can result from dietary deficiency, lack of sunlight, or lack of intestinal absorption of the vitamin such as occurs in celiac sprue and primary biliary cirrhosis.
- Certain medications can cause osteoporosis. These medicines include long-term use of heparin (a blood thinner), antiseizure medicine such as phenytoin and phenobarbital, and long-term use of oral corticosteroids (such as prednisone).
- Inherited disorders of connective tissue, including osteogenesis imperfecta, homocystinuria, osteoporosis-pseudoglioma syndrome, and skin diseases, such as Marfan syndrome and Ehlers-Danlos syndrome (These causes of hereditary secondary osteoporosis each are treated differently)
Complications of Osteoporosis and Osteopenia
The primary complication of osteoporosis is a bone fracture.
- This may lead to no symptoms or be associated with severe, intractable pain.
- Recurrent fractures are common and can lead to deteriorating skeletal structure.
- Occasionally, fractures of the spinal vertebrae can push bone into adjacent nerves and/or the spinal cord.
- This can require neurosurgical intervention.
- Osteoporotic vertebral fractures can also be relieved by vertebroplasty (kyphoplasty) procedures whereby the collapsed vertebra is inflated by a balloon and a cement (methylmethacrylate) is injected to reform the structure of the vertebra.
Repeated vertebral compression fractures can lead to severe deformity of the spine of the chest (kyphosis) that can compromise breathing along with cause extreme loss of height. This can increase the risk of problems with any respiratory infections.
Osteoporosis and Osteopenia signs symptoms
Osteoporosis an osteopenia can be present without any symptoms for decades because osteoporosis doesn’t cause symptoms until bone breaks (fractures). Moreover, some osteoporotic fractures may escape detection for years when they do not cause symptoms. Therefore, patients may not be aware of their osteoporosis until they suffer a painful fracture.
The symptom associated with osteoporotic fractures usually is pain.
Fractures of the spine (vertebra) can cause severe “band-like” pain that radiates from the back to the sides of the body. Over the years, repeated spinal fractures can lead to chronic lower back pain as well as loss of height and/or curving of the spine due to the collapse of the vertebrae. The collapse gives individuals a hunched-back appearance of the upper back, often called a “dowager hump” because it commonly is seen in elderly women.
A fracture that occurs during the course of normal activity is called a minimal trauma, or stress fracture. For example, some patients with osteoporosis develop stress fractures of the feet while walking or stepping off a curb.
Hip fractures typically occur as a result of a fall. With osteoporosis, hip fractures can occur as a result of trivial slip-and-fall accidents. Hip fractures also may heal slowly or poorly after surgical repair because of poor healing of the bone.

What factors determine bone strength?
Bone mass (bone density) is determined by the amount of bone present in the skeletal structure. Generally, the higher the bone density, the stronger the bones. Bone density is greatly influenced by genetic factors, which in turn are sometimes modified by environmental factors and medications. For example, men have a higher bone density than women, and African Americans have a higher bone density than Caucasian or Asian Americans.
- Normally, bone density accumulates during childhood and reaches a peak by around age 25.
- Bone density then is maintained for about 10 years. After age 35, both men and women will normally lose 0.3%-0.5% of their bone density per year as part of the aging process.
Estrogen is important in maintaining bone density in women. When estrogen levels drop after menopause, loss of bone density accelerates.
- During the first five to 10 years after menopause, women can suffer up to 2%-4% loss of bone density per year!
- This is predominantly attributed to insufficient estrogen and can result in the loss of up to 25%-30% of their bone density during that time period.
- Accelerated bone loss after menopause is a major cause of osteoporosis in women, referred to as postmenopausal osteoporosis. This is true even in women who seem to otherwise have normal health.
Who should have bone density testing?
The National Osteoporosis Foundation guidelines state that there are several groups of people who should consider DXA testing for proper diagnosis of bone health:
- All postmenopausal women below age 65 who have risk factors for osteoporosis
- All women aged 65 and older
- Postmenopausal women with fractures, although this is not mandatory because treatment may well be started regardless of bone density
- For women with any of more than 50 medical conditions associated with osteoporosis; a primary care physician can scan a patient’s list of medical illnesses to determine if one of these conditions is present.
- Women whose decision to begin treatment for osteoporosis might be aided by bone density testing to determine the presence or absence of osteoporosis or osteopenia.
The National Osteoporosis Foundation guidelines state that bone-density testing does not need to be performed if a person has a known osteoporotic fracture because the patient will be treated for osteoporosis with or without a bone-density study. In addition, bone-density testing is not appropriate if the person undergoing the test is not willing to take treatment based on the results. Therefore, if bone-density testing is done, it should be performed on people willing to take some specific action to improve their bone health based on the results.
SUBSCRIBE to dixecosmetics for Women’s Health Newsletter
Diagnosis of Osteoporosis and Osteopenia

A routine X-ray can reveal osteoporosis of the bone because the bones appear much thinner and lighter than normal bones. Unfortunately, by the time X-rays can detect osteoporosis, at least 30% of the bone has already been lost.
P.S: X-rays are not accurate indicators of bone density. Thus, the appearance of the bone on X-ray often is affected by variations in the degree of exposure of the X-ray film.
I (Dr Qaisar Ahmed) recommends a dual-energy X-ray absorptiometry scan (DXA, formerly known as DEXA) be used for the diagnosis of osteoporosis. DXA typically measures bone density in the hip, the spine, and the forearm.
The test takes only five to 15 minutes to perform, exposes patients to very little radiation (less than one-tenth to one-hundredth of the amount used on a standard chest X-ray), but still has lot of side effects.
The bone density of the patient is compared to the average peak bone density of young adults of the same sex and race. This score is called the “T score”, and it expresses the bone density in terms of the number of standard deviations (SD) below peak young adult bone mass.
- Osteoporosis is defined as a bone density T score of -2.5 or below.
- Osteopenia (between normal and osteoporosis) is defined as a bone density T score between -1 and -2.5.
It is important to note that while osteopenia is considered a lesser degree of bone loss than osteoporosis, it nevertheless can be of concern when it is associated with other risk factors (such as smoking, cortisone steroid usage, rheumatoid arthritis, family history of osteoporosis, etc.) that can increase the chances for developing vertebral, hip, and other fractures. In this setting, osteopenia may require medication as part of the treatment program.
How to treatment Osteoporosis and Osteopenia
The goal of the treatment of osteoporosis is the prevention of bone fractures by reducing bone loss or, preferably, by increasing bone density and strength. Although early detection and timely treatment of osteoporosis can substantially decrease the risk of future fractures, none of the available treatments for osteoporosis are complete cures
In allopathic drug therapy, it is impossible to completely rebuild bone that has been weakened by osteoporosis (in Homeopathy it is possible, see Homeopathic treatment below). The following are osteoporosis treatment and prevention measures for optimal health of the bone:
- Lifestyle changes, including quitting tobacco smoking, curtailing alcohol intake, exercising regularly, and consuming a balanced diet with adequate calcium and vitamin D.
- Allopathic drugs that stop bone loss and increase bone strength, such as alendronate, risedronate, raloxifene, ibandronate, calcitonin, zoledronate, and denosumab.
- Allopathic medications that increase bone formation such as teriparatide.

Calcium supplements for Osteoporosis and Osteopenia
Building strong and healthy bones requires an adequate dietary intake of calcium beginning in childhood and adolescence for both sexes. Most importantly, however, a high dietary calcium intake or taking calcium supplements alone is not sufficient in treating osteoporosis and should not be viewed as an alternative to or substituted for more potent prescription medications for osteoporosis. In the first several years after menopause, rapid bone loss may occur even if allopathic calcium supplements are taken; Here Homeopathic supplements works very good and without any side effects.
The allopathic calcium carbonate supplements are best taken in small divided doses with meals since the intestines may not be able to reliably absorb more than 500 mg of calcium all at once. Therefore, the best way to take 1,000 mg of a calcium supplement is to divide it into two doses. Likewise, a dosage of 1,500 mg should be split into three doses.
Side effects are indigestion, constipation, formation of calculi in kidneys, strangulation etc. Certain medications can interfere with the absorption of calcium carbonate for example: proton-pump inhibitors such as omeprazole, lansoprazole, lansoprazole, and rabeprazole, which are used in treating gastroesophageal reflux disease (GERD) or peptic ulcers. These p-p inhibitors also has too many side effects, some of those side effects could be fatal in old ages.
Vitamin D for Osteoporosis and Osteopenia
An adequate intake of calcium and vitamin D are important foundations for maintaining bone density and strength. However, calcium and vitamin D alone are not sufficient to treat osteoporosis and should be given in conjunction with other treatments. Vitamin D is important in several respects:
- Vitamin D helps the absorption of dietary calcium from the intestines. (watch on YouTube).
- The lack of vitamin D alone can cause calcium-depleted bone (osteomalacia), which further weakens the bones and increases the risk of fractures.
- Vitamin D, along with adequate calcium (1,200 mg of elemental calcium), has been shown in some studies to increase bone density and decrease fractures in postmenopausal women but not in premenopausal or perimenopausal women.
Vitamin D comes from the diet and the skin (sun light). Vitamin D production by the skin is dependent on exposure to sunlight. Active people living in sunny regions can produce most of the vitamin D they need in their skin. Conversely, lack of exposure to sunlight, due to residence in northern latitudes or physical incapacitation, causes vitamin D deficiency. In less temperate regions, production of vitamin D by the skin is markedly diminished in the winter, especially among the elderly.
An average multivitamin tablet contains 400 IU of vitamin D. Therefore, one to two multivitamins a day (beaver about the over dosage and side effects) should provide the recommended amount of vitamin D. Alternatively, vitamin D can be obtained in combination with calcium in tablet forms.
Chronic excessive use of vitamin D can lead to toxic levels of vitamin D, elevated calcium levels in blood and urine, and may also cause kidney stones.
Choosing an Osteoporosis and Osteopenia medication
In choosing a medication for osteoporosis, a physician will consider all aspects of a patient’s medical history as well as the severity of the osteoporosis.
If a postmenopausal woman has other menopausal symptoms such as hot flashes and vaginal dryness, HRT will be the proper choice for these menopausal symptoms as well as for the prevention of osteoporosis. After the menopausal symptoms have passed, some other non estrogen prescription medication will be considered for the longer term.
If the prevention and treatment of osteoporosis is the only issue under consideration, then bisphosphonates such as alendronate, ibandronate, or risedronate are more effective than menopausal hormone therapy in preventing osteoporotic fractures and less likely to be associated with substantial adverse effects. So far, bisphosphonates are the most well-studied and effective category of prescription medication for treating postmenopausal osteoporosis.
A few serious esophageal conditions preclude the use of oral bisphosphonates, specifically esophageal stricture or achalasia. In these two conditions, it is likely that the bisphosphonate tablets will be retained in the esophagus and lead to esophageal inflammation, ulceration, and scarring. Caution often is advised for people with dysphagia (trouble swallowing) because the dysphagia may be a manifestation of a problem in the esophagus that will cause the bisphosphonate tablets to get stuck.
Caution also is advised when there is gastritis, duodenitis, or ulcers because of the possibility that the bisphosphonate will aggravate the inflammation associated with these conditions. Any worsening of gastrointestinal symptoms should be reported immediately, but the vast majority of people tolerate bisphosphonates without symptoms when the prescribing directions are followed carefully.
Prescribing directions should be followed carefully. Moreover, intravenous bisphosphonates, such as zoledronate or injectable denosumab, may be given to those with esophageal strictures, achalasia, dysphagia, or gastrointestinal side effects from oral bisphosphonates.
In patients with GERD or who have symptoms of heartburn, risedronate and alendronate may prove to cause irritation to the esophagus, intravenous bisphosphonates, such as zoledronate may be preferred.
Calcitonin is a weaker antiresorptive medication than bisphosphonates. It is reserved for patients who cannot take or will not consider taking other medications. Raloxifene also is a weaker medication for improving bone density or preventing fractures as compared to estrogen or bisphosphonates. In patients with moderate to severe osteoporosis, it is advisable to use the more potent antiresorptive medications (bisphosphonates). In addition, the safety and effectiveness of more than three years of raloxifene, or more than 24 months of teriparatide, have not been well studied.
Estrogen replacement and raloxifene differ in their side effects and also in their effects on cholesterol levels. For example, raloxifene does not raise the “good” HDL cholesterol but estrogen replacement does. Both estrogen and raloxifene lower the “bad” LDL cholesterol.
Watch on YouTube click Here.
Medications that prevent bone loss and breakdown
Currently, the most effective medications for osteoporosis are antiresorptive agents, which decrease the removal of calcium from bones. The bone is a living dynamic structure; it is constantly being built and removed (resorbed). This process is an essential part of maintaining the normal calcium level in the blood and serves to repair tiny cracks in the bones that occur with normal daily activity and remodel bone based on the physical stresses placed on the bone. Osteoporosis results when the rate of bone resorption exceeds the rate of bone rebuilding.
Antiresorptive medications inhibit the removal of bone (resorption), thus tipping the balance in favor of bone rebuilding and increasing bone density.
Bisphosphonates
Bisphosphonates decrease the risk of hip fracture, wrist fracture, and spine fracture in people with osteoporosis and can improve the T-score.
To reduce side effects (like liver diseases, renal and gastric diseases, cancers, Thrombosis, DVT etc.) and to enhance absorption of the medicine, all bisphosphonates taken by mouth (orally) should be taken in the morning, on an empty stomach, 30 minutes before breakfast, and with at least 8 ounces (240 ml) of water (not juice). This improves the absorption of the bisphosphonate. Taking the pill sitting or standing (as well as drinking adequate amounts of liquids) minimizes the chances of the pill being lodged in the esophagus, where it can cause ulceration and scarring. Patients should also remain upright for at least 30 minutes after taking the pill to avoid reflux of the pill into the esophagus. Newer intravenous bisphosphonates, such as ibandronate and zoledronate, bypass the potential esophagus and stomach problems.
Food, calcium, iron supplements, vitamins with minerals, or antacids containing calcium, magnesium, or aluminum can reduce the absorption of oral bisphosphonates, thereby resulting in loss of effectiveness. Therefore, oral bisphosphonates should be taken with plain water only in the morning before breakfast. Also, no food or drink should be taken for at least 30 minutes afterward.
Alendronate
Alendronate is a bisphosphonate antiresorptive medication. Alendronate is approved for the prevention and treatment of postmenopausal osteoporosis as well as for osteoporosis that is caused by cortisone-related medications (glucocorticoid-induced osteoporosis). Alendronate has been shown to increase bone density and reduce fractures in the spine, hips, and arms. Fosamax is taken by mouth once a week to prevent and treat postmenopausal osteoporosis. Alendronate is the first osteoporosis medication also approved for increasing bone density in men with osteoporosis, either in a daily or a weekly dosing schedule.
Alendronate generally is well tolerated but with may side effects. One side effect of alendronate is irritation of the esophagus (the food pipe connecting the mouth to the stomach). Inflammation of the esophagus (esophagitis) and ulcers of the esophagus, liver intoxication, renal failure and calculies, cancer etc, have been reported infrequently with alendronate use.
Risedronate
Risedronate is another bisphosphonate antiresorptive medication. Like alendronate, this drug is approved for the prevention and treatment of postmenopausal osteoporosis as well as for osteoporosis that is caused by cortisone-related medications (glucocorticoid-induced osteoporosis). Risedronate is chemically different from alendronate but with almost the same side effects.
Ibandronate
Ibandronate is a bisphosphonate for the prevention and treatment of postmenopausal osteoporosis. It is available in formulations for both daily and monthly oral use as well as for intravenous use every three months.
Zoledronate
Zoledronate is a unique intravenous bisphosphonate antiresorptive medication that is given once every year. This formulation seems to have good ability to strengthen bones and prevent fractures of both spinal and non spinal bones. The convenience of once-a-year dosing is obvious. As with all bisphosphonates, patients taking Reclast must be taking adequate calcium and vitamin D prior to and after infusion of the medication for optimal results.
Generally, patients are given acetaminophen the day of the infusion and for several days afterward to prevent occasional minor muscle and joint aches. The infusion lasts approximately 20-30 minutes. Reclast is used to treat and prevent osteoporosis in postmenopausal women and increases bone mass in men with osteoporosis. Zoledronate also used to treat and prevent steroid-induced osteoporosis (glucocorticoid-induced osteoporosis). Zoledronate reduces the risk of fractures after a low-trauma hip fracture. Reclast should not be used in patients who have had avascular necrosis or during/prior to pregnancy (due to its sever side effects like cancers. DVT etc.).
Selective estrogen receptor modulators (SERMs)
Raloxifene
Raloxifene belongs to a class of drugs called selective estrogen receptor modulators (SERMs). SERMs work like estrogen in some tissues but as an antiestrogen in other tissues. The SERMs were developed to reap the benefits of estrogen while avoiding the potential side effects of estrogen. Thus, raloxifene can act like estrogen on the bone but as an antiestrogen on the lining of the uterus where the effects of estrogen can promote cancer.
The first SERM to reach the market was tamoxifen, which blocks the stimulative effect of estrogen on breast tissue. Tamoxifen has proven valuable in women who have had cancer in one breast for preventing cancer in the second breast but unfortunately with too many side effects.
Raloxifene has been approved for the prevention and treatment of osteoporosis in postmenopausal women. In a three-year study involving some 600 postmenopausal women, raloxifene was found to increase bone density (and lower LDL cholesterol) while having very few detrimental effect on the uterine lining (which means that there are very little chances to cause uterine cancer).
Because of its antiestrogens effects, the most common side effects with Raloxifene are hot flashes. Conversely, because of its estrogenic effects, Raloxifene increases the risk of blood clots, including deep vein thrombosis (DVT) and pulmonary embolism (blood clots in the lung). The greatest increase in risk occurs during the first four months of use.
Patients taking raloxifene should avoid prolonged periods of immobility during travel when blood clots are more prone to occur. The risk of deep vein thrombosis with raloxifene is probably comparable to that of estrogen, about two to three times higher than the usual low rate of occurrence. Raloxifene decreases the risk of spinal fractures in postmenopausal women with osteoporosis, but it is not known if there is a similar benefit in decreasing the risk of hip fracture.
Calcitonin
Calcitonin is a hormone that has been approved for treating osteoporosis. Calcitonins come from several animal species, but salmon calcitonin is the one most widely used. Calcitonin can be administered as a shot under the skin (subcutaneously), into the muscle (intramuscularly), or inhaled nasally (intranasally). Intranasal calcitonin is the most convenient of the three methods of administration.
Calcitonin has been shown to prevent bone loss in postmenopausal women. In women with established osteoporosis, calcitonin has been shown to increase bone density and strength in the spine only.
Calcitonin is a weaker antiresorptive medication than bisphosphonates. Calcitonin is not as effective in increasing bone density and strengthening bone as estrogen and other antiresorptive agents, particularly bisphosphonates. In addition, it is not as effective as bisphosphonates in reducing the risk of spinal fractures and has not been proven effective in reducing hip fracture risk. Therefore, calcitonin is not the first choice of treatment in women with established osteoporosis. Nevertheless, calcitonin is a helpful alternative treatment for patients who cannot tolerate other medications.
Teriparatide
Teriparatide is a synthetic version of the human parathyroid hormone, which helps to regulate calcium metabolism. Unlike other medications for osteoporosis that reduce the resorption of bone, teriparatide very effectively promotes the growth of new bone. Forteo is self-injected into the skin. Because long-term safety is not yet established, it is only approved for 24 months of use. It reduces spinal fractures in women with known osteoporosis, but it is not known if there is a similar reduction in the risk for hip fracture. Generally, after a two-year course of teriparatide, the patient is switched to bisphosphonate therapy to maintain bone density.
Denosumab
The latest treatment approved for osteoporosis is denosumab, an injectable antibody that blocks a chemical messenger that plays a role in promoting bone thinning by the bone cells that are responsible for bone resorption. Prolia strengthens bone by increasing its density and reducing fractures. Prolia is administered by twice yearly injections under the skin. Denosumab is used for the treatment of postmenopausal women with osteoporosis at high risk for fracture, defined as a history of osteoporotic fracture, multiple risk factors for fracture, or patients who have failed or are intolerant to other available osteoporosis therapy. Denosumab can cause an increased risk of infections and low blood calcium levels (hypocalcemia).
Hormone therapy (menopausal hormone therapy)
Estrogen hormone therapy after menopause (previously referred to as hormone replacement therapy or HRT) has been shown to prevent bone loss, increase bone density, and prevent bone fractures. It is useful in preventing osteoporosis in postmenopausal women. Estrogen is available orally or as a skin patch.
Estrogen also is available in combination with progesterone as pills and patches. Progesterone is routinely given along with estrogen to prevent uterine cancer that might result from estrogen use alone. Some doctors thinks that women who have had a hysterectomy (surgical removal of the uterus) may take estrogen alone since they no longer have a uterus to become cancerous, but it is not proven as some of patients developed breast and rectal cancers.
Nasally delivered estrogen and lower-dose combination pills of estrogen and progesterone are also being studied. However, due to adverse effects of HRT, such as increased risks of heart attack, stroke, blood clots in the veins, and breast cancer; HRT is no longer recommended for long-term use in the therapy of osteoporosis. Rather, HRT is used short-term to relieve menopausal hot flashes.
Every woman needs to have an individualized discussion regarding HRT with her doctor because each woman will place a different weight on the risks and benefits of the treatment.
Monitoring osteoporosis therapy
The controversy of bone density testing in patients already taking osteoporosis medication
Repeat bone density testing (DXA scans) not be done for monitoring osteoporosis treatment or prevention on a routine basis. It is sometimes difficult to know just how to use repeated bone density measurements during therapy. Here are a few of the most important reasons:
- Bone density changes so slowly with treatment that the changes are smaller than the measurement error of the machine. In other words, repeat DXA scans cannot distinguish between a real increase in bone density due to treatment and a mere variation in measurement from the machine itself.
- The real purpose of osteoporosis treatment is to decrease future bone fractures. There is no good correlation between increases in bone density with decreases in fracture risks with treatment. For example, alendronate has been shown to decrease fracture risk by 50% but only to increase bone density by a few percent. In fact, most of the fracture reduction with raloxifene is not explained by raloxifene’s effects on bone mineral density.
- One density measurement taken during treatment will not help the doctor plan or modify treatment. For example, even if the DXA scan shows continued deterioration in bone density during treatment, there is not yet research data demonstrating that changing a medication, combining medications, or doubling medication doses will be safe and helpful in decreasing the future risk of fractures.
- Even if bone density deteriorates during treatment, it is quite likely that the patient would have lost even more bone density without treatment.
- Recent research has shown that women who lose bone density after the first year of HRT will gain bone density in the next two years of therapy, whereas women who gain in the first year will tend to lose density in the next two years of therapy. Therefore, bone density during treatment fluctuates naturally, and these fluctuations may not correlate with the prevention of fractures due to the medication.
Controversy
Currently, it is not clear how long patients with osteoporosis are treated with allopathic bisphosphonates and should continue the bisphosphonate treatment. Many allopathic doctors are interrupting treatment for a “drug holiday” off of the drug as it may not be necessary after five to seven years. Guidelines for the duration of treatment of osteoporosis with bisphosphonates are being developed.
Homeopathic Treatment
Compared to allopathic treatment, Homeopathic treatment is shorter and more effective, and more importantly, there are no side effects of Homeopathic medicines.
Here are few of Homeopathic medicines for osteoporosis, always advise them along with other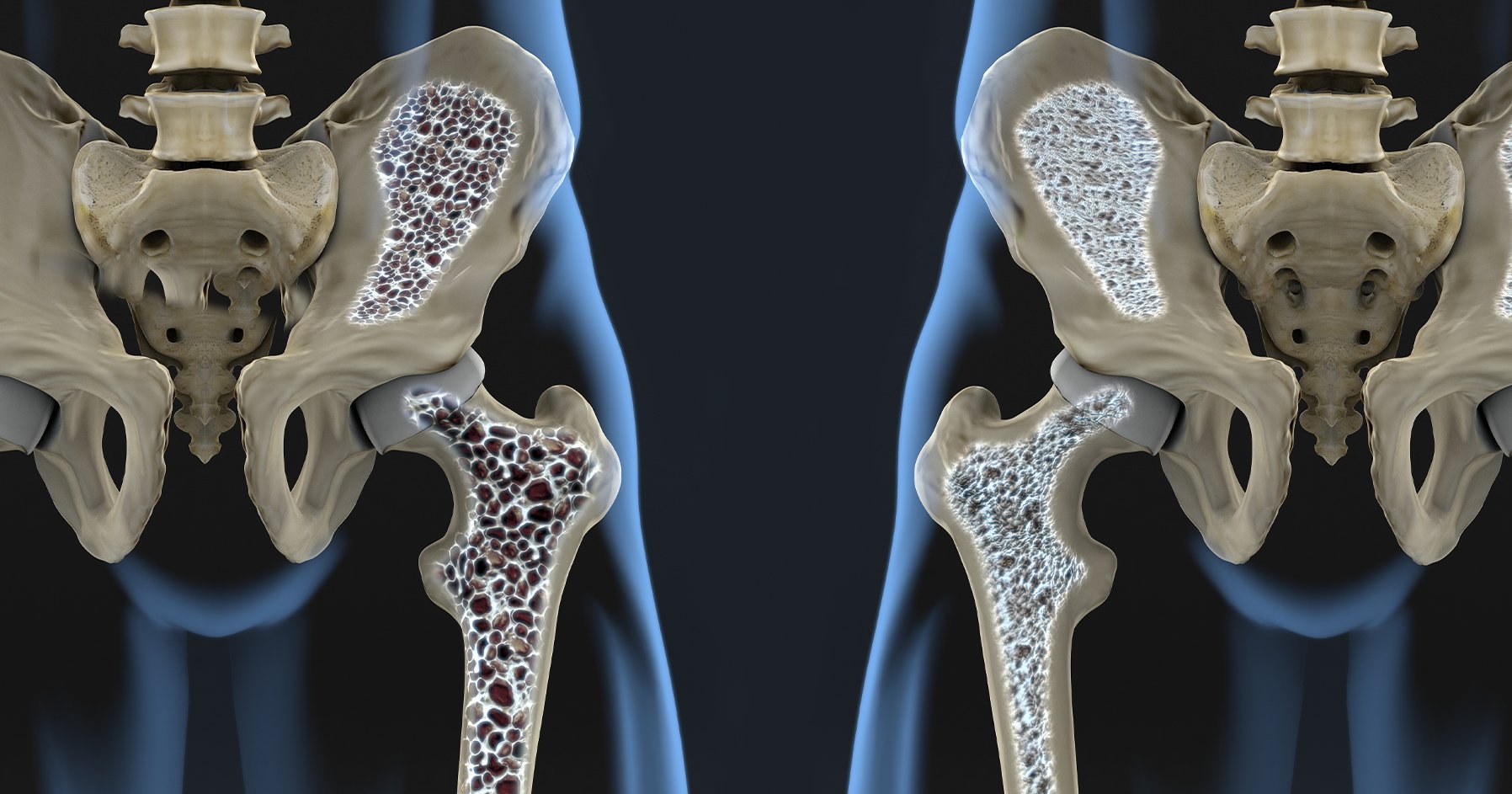 constitutional medicines.
constitutional medicines.
Silicia
Weak spine; very susceptible to draughts on back. Pain in coccyx. Spinal irritation after injuries to spine; diseases of bones of spine. Potts’ disease. Bones are sensitive and tender to touch. Sciatica, pains through hips, legs and feet. It is accompanied with pain on touch and movement. Burning sensation in the back. It gets worse in open air. Silicea can be taken when a person has pain in lower back on stooping and on rising from a seat. Drawing, tearing, and shooting in limbs, shooting in all joints. Silicea is very helpful in the efficient union of broken bone it also helps in removing bone splinters.
Symphytum Officinale
A best choice for treating fractures in osteoporosis. It is commonly known as ‘knit bone’ and as the name represents it helps in knitting/uniting the fractured bone, it helps in joining fractured bones very efficiently by promoting the activity of fibroblast cells. Fractures, where patients complain of pricking pain at the fractured site, It also help in reducing irritability at the site of fracture. Pott’s disease from fall. Caries (weakness/osteoporosis)of spinal and other bones. Symphytum acts specially on the joints in elder (menopaused) ladies.
Phosphorus
Phosphorus can give best results in curvature of spine along with burning sensation in the spine. Weakness in all the limbs as if paralysed; especially in joints, trembling from every exertion. Swelling of hands and feet. Bruised pain in limbs -Extremities, especially hands and feet.
Calcarea Phosphorica
Throbbing or jerking pains below scapula. Violent pain in region of back when making the least effort. Weak, soft, brittle bones which become crooked. It improves bone strength. Sharp pains in sacrum and coccyx. Soreness as if separate in sacroiliac synchondrosis. Curvature of the spine, pain in the hip bone. The pain can be shooting, drawing, stitching or tearing in nature. Calcarea Phos is also beneficial for those experiencing pain in the back due to weak bones. The pain may get worse from the least movement. Gouty nodosities. Soreness, torpor, and paralysis. Soreness of tendons.
Calcarea Carbonica
Rigidity of the neck. Hard and strumous swelling of the thyroid gland. It is found to be effective in improving bone health and strengthening bones. Drawing/crawling pains in the arms. Sudden attacks of paralytic weakness in limbs. Drawing lancinations, or incisive, acute pains in the hips and in the thighs. Dislocation of the hips. knees joints.
Asafoitida
Darting pain and caries in bones. Periosteum painful, swollen, enlarged. Ulcers affecting bones; thin, ichorous pus.
Mezerium
Pain in neck and back; worse, motion and at night; intolerant of all touch. Pain and burning in tibia and long bones. Legs and feet tingling. Pain in hip and knee. Dislocating joints. Tension and stiffness in knees. Jerking, and pressive pain in tibia. Hard swelling of calves of legs. Jerking pain in toes. Violent pains in bones of feet.
Ruta
Spine and limbs feel bruised. Small of back and loins pain. Legs weakness. Fractures in osteoporosis. Ganglia (Benzoic ac). Sciatica; worse, lying down at night. Damaged tendons. Helps in healing torn tendons and ligaments. It also helps in repairing the damaged bone. Aching pain in tendo-Achilles. Thighs pain when stretching the limbs. Pain in bones of feet and ankles, pain, soreness, and stiffness around the fractured area mainly wrist fracture.
Hypericum
Darting pain in shoulders. Pressure along ulnar side of arm. Cramp in calves. Pain in toes and fingers, especially in tips. Crawling in hand and feet. Lancinating pain in upper and lower limbs. Neuritis, with tingling, burning pain, numbness and flossy skin. Joints feel bruised. Hysterical joints. Pain in the back due to crushing of nerves in between damaged vertebral bones. The excessive pain and sensitivity in the back after fracturing of vertebral bones that gets worse by the slightest motion of the neck or arms. Pressure over sacrum. Spinal concussion. Coccyx injury from fall, with pain radiating up spine and down limbs.
Symphytum Officinale
Wounds penetrating to perineum and bones, and in non-union of fractures; irritable stump after amputation, irritable bone at point of fracture. Psoas abscess. Pricking pain and soreness of periosteum. Inflammation of inferior maxillary bone. Pott’s disease from fall. Loss of power in the large joints in elder patients. Inflammation of bones.
Prevention of hip fractures in elderly people with Osteoporosis and Osteopenia
Elderly people with osteoporosis can decrease their risk for hip fracture by maintaining muscle strength, coordination, and balance with exercise programs. Throw rugs and animals in pathways of the home should be minimized or eliminated. Good lighting is essential for safe walking to the restroom both day and night.
Additionally, for those elderly people who use canes for walking, etc., it is essential that the rubber tips of the canes are regularly checked for any signs of wear. When this rubber wears through it presents a serious risk of causing the cane (and, therefore, the person) to slip, which can result in serious bodily harm — including hip fracture.
Prognosis with allopathic Osteoporosis and Osteopenia treatment
The outlook for patients with osteoporosis depends greatly on where fractures occur. Additionally, if treatment is begun when the bone disease is detected early, the outcome is better.
Newer medications, medicine with different methods of delivery, and research into the optimal management of osteoporosis will bring even better options for the healthcare of patients with osteoporosis in the future.
P. S : This article is only for doctors having good knowledge about homeopathy, and for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
Location, address and contact numbers are given below.
NoN of above mentioned medicine(s) is/are not the full/complete treatment, but just hints for treatment; every patient has his own constitutional medicine along with these mentioned above.
To order medicine by courier, please send your details at WhatsApp– +923119884588
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS) ; senior research officer Dnepropetrovsk state medical academy Ukraine; is a leading Homeopathic physician practicing in Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS) ; senior research officer Dnepropetrovsk state medical academy Ukraine; is a leading Homeopathic physician practicing in Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr. Sayyad Qaisar Ahmed at :
https://www.youtube.com/Dr Qaisar Ahmed