
Tuberculosis (TB) is a multi systemic infectious disease caused by Mycobacterium tuberculosis (or TB, TB germs), a rod-shaped bacterium.
Thank you for reading this post, don't forget to subscribe!Tuberculosis (TB may stand for the disease or the bacteria that cause the disease) is the most common cause of infectious disease-related mortality worldwide (about 10 million people worldwide were sick with TB in 2017, and about 1.3 million people died from TB worldwide in 2017 according to the World Health Organization [WHO] and the CDC).
HIV-associated Tuberculosis infections are a leading cause of death. TB symptoms can span such a wide range that TB is termed the “great imitator” by many who study infectious diseases because TB symptoms can mimic many other diseases.
Additional terms describe TB include consumption, Pott’s disease, active, latent, pulmonary, cutaneous, and others, and they appear in both medical and nonmedical publications. In most instances, the different terms refer to a specific type of TB with some unique symptoms or findings. The most common site (about 85%) for TB to develop is in the pulmonary tract although it may infect other parts of the body. Humans are not the only known hosts for Mycobacterium tuberculosis, it can infect animals. The bacteria may stain weakly both gram-negative and gram-positive due to their cell surface so medical professionals use acid-fast stains to visualize the cells with a microscope.
Mycobacterium tuberculosis (mycobacteria or TB) are slow-growing, aerobic, and can grow within body cells (an intracellular parasitic bacterium). Its unique cell wall helps protect it from the body’s defenses and gives mycobacteria the ability to retain certain dyes like fuchsin (a reddish dye) after an acid rinse that rarely happens with other bacterial, fungal, or parasitic genera.
Mycobacteria that escape destruction by immune system may be spread by blood or lymphatic pathways to most organs, with a preference for those that oxygenate well (for example lungs, kidneys, and bones). Typical TB lesions, termed granulomas, usually consist of a central necrotic area, then a zone with macrophages, giant Langerhans cells, and lymphocytes that become surrounded by immature macrophages, plasma cells, and more lymphocytes. These granulomas also contain mycobacteria. In latent infections, a fibrous capsule usually surrounds the granulomas, and in some people, the granulomas calcify, but if the immune defenses fail initially or at a later time (reactivate), the bacteria continue to spread and disrupt organ functions.
Types of tuberculosis (TB)
There are many types of tuberculosis, but the main two types are termed either active or latent tuberculosis infection.
Active TB is when the disease is actively producing symptoms and can be contagious (transmitted to other people).
Latent disease is when the person is infected with Mycobacterium tuberculosis bacteria, but the bacteria are not producing symptoms (usually due to the body’s immune system suppressing the bacterial growth and spread) and have no TB bacteria in the sputum.
Patients with latent TB usually cannot transfer Mycobacterium tuberculosis bacteria to others unless the immune system fails; the failure causes reactivation (bacterial growth is no longer suppressed) that results in active TB so the person becomes contagious. Latent TB resembles a chickenpox infection that goes dormant and may reactivate years later.
Many other types of TB exist in either the active or latent form. These types are named for the signs and the body systems Mycobacterium tuberculosis preferentially infect, and these infection types vary from person to person. Consequently, pulmonary tuberculosis mainly infects the pulmonary system (lungs), cutaneous TB has skin symptoms, while miliary TB describes widespread small infected sites (lesions or granulomas about 1 mm-5 mm) found throughout body organs. It is not uncommon for some people to develop more than one type of active TB. More types will be listed in the symptoms and signs section below.
Atypical mycobacteria that may cause disease are the Mycobacterium Avium complex, Mycobacterium Fortuitum complex, and Mycobacterium Kansasii.
There are three stages of tuberculosis
Primary infection:
The bacteria enters the body as we breathe. In the early weeks, the bacilli travel to the regional lymph nodes and enter the bloodstream. The infection may then spread to other parts of the body like lungs, bones, kidneys and meninges of the brain. However, this is less likely in patients who have been vaccinated or have had a prior infection.
Latent infection:
This occurs after primary infection. In 95% of cases, a person’s immune system suppressed TB bacteria (preventing it from multiplying). This leads to the disappearance of symptoms even though a small amount of M.tb is still present in the person’s body.
Active disease:
This stage occurs when the latent disease reactivated or if the patient gets re-infected A person infected with tuberculosis may not have any specific symptoms (latent TB) or may present with symptoms (active TB) such as persistent cough with sputum for more than two weeks, low-grade fever, chills, breathlessness, enlarged lymph nodes, fatigue, weight loss, loss of appetite, coughing up blood and night sweats.
Risk factors for tuberculosis
Tuberculosis usually spread between people who are in close contact (working and/or living together).
There are many risk factors for developing tuberculosis, such as people who work in hospitals and other areas where TB-infected people may reside (jails, nursing homes, group homes for HIV patients, homeless shelters).
Other people at high risk include the following:
- Visitors and immigrants from areas known to have a high incidence of TB
- Children and the elderly with weakened immune systems (especially those with a positive TB skin test, see below)
- Patients with HIV infection
- Drug abusers, especially IV drugs
- Head and neck cancer patients
- Transplant patients
- Diabetics
- Kidney disease patients
- People undergoing immunosuppressive therapy (allopathic)
- Silicosis
- Close association with drug users or people with known TB infections are also at higher risk.
Symptoms
Although there are several TB types, pulmonary tuberculosis is responsible for the majority (about 85%) of TB infections. Consequently, pulmonary TB symptoms and signs may occur with or even before other types of TB are diagnosed.
The classical clinical signs and symptoms of pulmonary TB may include the following:
- Fever
- Night sweats
- Cough (often chronic)
- Hemoptysis (coughing up bloody sputum)
- Decrease or loss of appetite
- Weight loss and/or muscle loss (unintentional)
- Fatigue and/or malaise
- Chest pain (pain while breathing)
- Shortness of breath
- Swollen lymph nodes
- Pneumonitis (maybe the only symptom in the elderly).
Other types are loosely classified as extrapulmonary and often have symptoms that are nonspecific but frequently localized to the involved site.
The following includes the signs and symptoms of additional types of TB:
- Skeletal TB (also termed Pott’s disease): spinal pain, back stiffness, and paralysis is possible
- TB meningitis: headaches (variable in length but persistent), mental changes, coma
- TB arthritis: usually pain in a single joint (hips and knees most common)
- Genitourinary TB: dysuria, flank pain, increased frequency, masses or lumps (granulomas)
- Gastrointestinal TB: difficulty swallowing, nonhealing ulcers, abdominal pain, malabsorption, diarrhea (may be bloody)
- Miliary TB: many small nodules widespread in organs that resemble millet seeds (hence its name)
- Pleural TB: empyema and pleural effusions
- Multidrug-resistant tuberculosis (MDR TB)
- XDR or extensively drug-resistant TB: patients infected with TB bacteria that are resistant to some of the most effective anti-TB medications (XDR stands for extensively drug-resistant)
- Caseous TB: Necrotic (dead and dying) tissue that is infected with TB organisms has a soft, dry, and cheesy appearance.
- End-stage TB: Patients may suffer fever, constant coughing, shortness of breath, weight loss, mental changes, and blood in their sputum before death.
Diagnose tuberculosis
Because TB may occur as either a latent or active form, the definitive diagnosis of active tuberculosis depends on the culture of mycobacteria from sputum or tissue biopsy. However, it may take weeks for these slow-growing bacteria to grow on specialized media.
Since patients with latent TB do not require isolation or immediate drug therapy, it is useful to determine if a person is either not infected, has a latent infection, or is actively infected with transmissible TB bacteria. Consequently, doctors needed a presumptive test(s) that could reasonably assure that the person was infected or not.
After getting a patient’s history and physical exam data, the next usual test is the skin test known as the Mantoux tuberculin skin test or the tuberculin skin test or TST, sometimes referred to as a PPD test.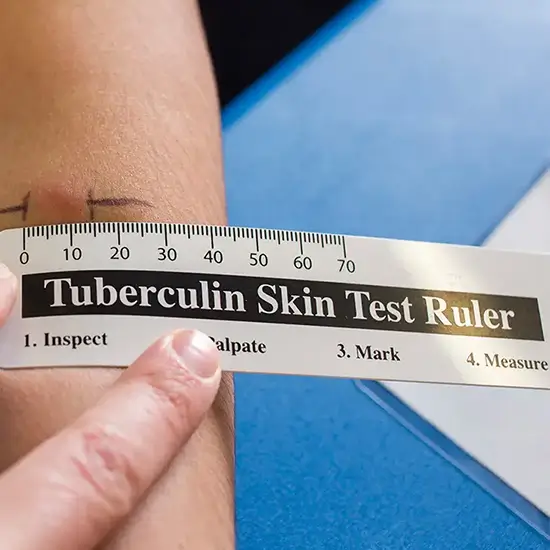
The test involves injecting tuberculin (an extract made from killed mycobacteria) into the skin. In about 48-72 hours, the skin is examined for induration or swelling by a doctor; a positive test (induration) strongly suggests the patient has either been exposed to live mycobacteria or is actively infected (or had been vaccinated); no induration suggests the person tests negative for TB.
This test can have false-positive results especially in individuals vaccinated for TB with the BCG vaccine. False-negative results can be caused by patients who are immunocompromised.
Another test, IGRA (interferon-gamma release assays) can measure the immune response to Mycobacterium tuberculosis.
Chest X-rays can give evidence of lung infection while a sputum smear stained with certain dyes that are retained mainly (but not exclusively) by mycobacteria can show the presence of the bacterium. These tests, when examined by a doctor, are useful in establishing a presumptive diagnosis of either latent or active TB, and most doctors will initiate treatment based on their judgment of these tests.
In addition, some of these tests are useful in people who are not vaccinated with a TB vaccine but are less useful in vaccinated people. For some patients, culture studies still should be completed to determine the drug susceptibility of an infecting TB strain.
Other tests for example, a PCR test (polymerase chain reaction) to detect TB antigens and the LED-FM microscopic technique to identify TB organisms with microscopy may be used. Two other TB blood tests (also called interferon-gamma release assays or IGRAs) have been approved by the FDA and measure how strongly the body’s immune system reacts to TB bacteria. IGRAs are recommended in testing patients who have been vaccinated against TB (see prevention section below).
People with positive symptoms, positive blood tests, sputum smear, or culture-positive are considered infected with TB and contagious (active TB).
Physicians diagnose and treat people with latent TB infections (LTBI) according to the following current CDC criteria:
- No symptoms or physical findings suggestive of TB disease
- TST or IGRA result is usually positive
- A chest radiograph is typically normal
- If done, respiratory specimens are smeared and culture-negative
- Cannot spread TB bacteria to others
- Should consider treatment for LTBI to prevent TB disease (strongly advised by the CDC)
Allopathic Treatment for Tuberculosis
The treatment for TB depends on the type of TB infection and drug sensitivity of the mycobacteria. For latent TB, three anti-TB drugs are used in four different recommended schedules. The drugs are isoniazid, rifampin (Rifadin), and rifapentine (Priftin) and the CDC’s four recommended schedules are below and are chosen by the treating doctor based on the patient’s overall health and type of TB the patient was likely exposed to.
| Drugs | Duration | Interval | Minimum Doses |
|---|---|---|---|
| Isoniazid | 9 months | Daily Twice weekly |
270 76 |
| Isoniazid | 6 months | Daily Twice weekly |
180 52 |
| Isoniazid and Rifapentine | 3 months | Once weekly | 12 |
| Rifampin | 4 months | Daily | 120 |
First-line drugs used to treat active TB are INH, RIF, ethambutol (EMB; Myambutol), and pyrazinamide. A guide for the basic treatment schedules for active TB (drug-susceptible TB organisms) as follows:
| Preferred Regimen | Alternative Regimen | Alternative Regimen | |
|---|---|---|---|
| *EMB can be discontinued if drug susceptibility studies demonstrate susceptibility to first-line drugs. | |||
| Initial Phase Daily INH, RIF, PZA, and EMB* for 56 doses (8 weeks) |
Initial Phase Daily INH, RIF, PZA, and EMB* for 14 doses (2 weeks), then twice weekly for 12 doses (6 weeks) |
Initial Phase Thrice-weekly INH, RIF, PZA, and EMB* for 24 doses (8 weeks) |
|
| Continuation Phase Daily INH and RIF for 126 doses (18 weeks) or twice-weekly INH and RIF for 36 doses (18 weeks) |
Continuation Phase Twice-weekly INH and RIF for 36 doses (18 weeks) |
Continuation Phase Thrice-weekly INH and RIF for 54 doses (18 weeks) |
|
The most current treatment guidelines need to be reviewed and correlated to the patient’s specific condition and circumstances before any treatment are started.
Corticosteroids are sometimes used to treat TB when inflammation is a major cause of morbidity and are indicated for patients with acute respiratory distress syndrome or closed-space infections, such as meningitis and pericarditis. Dexamethasone 12 mg orally or IV every 6 hours is given to adults and children > 25 kg; children < 25 kg are given 8 mg. Treatment is continued for 2 to 3 weeks. Corticosteroids that are needed for other indications pose no danger to active TB and patients who are receiving an effective TB regimen.
are indicated for patients with acute respiratory distress syndrome or closed-space infections, such as meningitis and pericarditis. Dexamethasone 12 mg orally or IV every 6 hours is given to adults and children > 25 kg; children < 25 kg are given 8 mg. Treatment is continued for 2 to 3 weeks. Corticosteroids that are needed for other indications pose no danger to active TB and patients who are receiving an effective TB regimen.
Treatment of drug-resistant (or antibiotic-resistant) and multi-drug-resistant tuberculosis TB can be difficult. These TB patients may require second-line drugs. Patients with these infections are recommended to involve infectious-disease specialists as multiple approaches involve other anti-TB drugs and variable treatment schedules that can be used.
The infectious-disease consultant may be aware of the newest treatments that may benefit specific patients. For example, bedaquiline (Sirturo) has been approved for the treatment of MDR TB, and research with an antimicrobial drug, moxifloxacin, suggests it may help in treatment protocols.
Some serious side effects of allopathic treatment may include the following:
- Loss of appetite
- Gastric ulcers
- Gastritis and Nausea and/or vomiting
- Liver weakness
- Jaundice
- Low hemoglobin levels
- Renal complications
- Paresthesia
- Bruise formation, bleeding
- Vision changes
In some patients, the lung destruction may be severe and the only treatment left may be surgical resection of the diseased lung tissue.
Medications are needed for TB treatment. Diet regime helps reduce symptoms.
Homeopathic Treatment for Tuberculosis
Tuberculinum
Undoubted value in the treatment of incipient tuberculosis. Patient always tired; motion causes intense fatigue; aversion to work; wants constant changes. When symptoms are constantly changing and well-selected remedies fail to improve, and cold is taken from the slightest exposure. Rapid emaciation. Of great value in epilepsy, neurasthenia and in nervous children. Diarrhoea in children running for weeks, extreme wasting, bluish pallor, exhaustion. Mentally deficient children. Enlarged tonsils. Skin affections, acute articular rheumatism. Very sensitive, mentally and physically. General exhaustion. Nervous weakness. Trembling. Epilepsy. Arthritis.
Enlarged tonsils. Hard, dry cough during sleep. Expectoration thick, easy; profuse bronchorrhea. Shortness of breath. Sensation of suffocation, even with plenty of fresh air. Longs for cold air. Broncho-pneumonia in children. Hard, hacking cough, profuse sweating and loss of weight, rales all over chest. Deposits begin in apex of lung. Putrid ulcers, surrounded by little pimples.
Hepar Sulph
Suits especially scrofulous and lymphatic constitutions who are inclined to have eruptions and glandular swellings. Unhealthy skin, Sweating, Respiratory mucous membrane, producing croupous catarrhal inflammation, profuse secretion; also easy perspiration. Sinus with pus forming, Chilliness, hypersensitiveness, splinter-like pains. Corneal nonhealing ulcers. Dry cough, choking cough, rattling, croaking cough; suffocative attacks of cough. Abscesses; suppurating glands are very sensitive. Papules. Ulcers, with bloody suppuration.
Hydrastis Canadensis
Acts especially on mucous membranes, relaxing them and producing a thick, yellowish, ropy secretion, yellow, tenacious mucus , throat, stomach, uterus, urethra,-it is always characterized by this peculiar mucous discharge. Chest raw, sore, burning. Dry, harsh cough. Bronchitis.
Easily-tired people, cachectic individuals, with great debility. Cerebral effects prominent, weak muscular power, poor digestion and obstinate constipation. Lumbago. Emaciation and prostration. Cancer and cancerous state, before ulceration. Goitre of puberty and pregnancy.
Weak digestion. Atonic dyspepsia. Ulcers and cancer. Gastritis. Gastro-duodenal catarrh. Liver torpid, tender. Jaundice. Eruption like variola. Lupus; ulcers, cancerous formations. General tendency to profuse perspiration and unhealthy skin.
Stannum Metallicum
Mucus expelled by forcible cough. Violent, dry cough in evening until midnight. Cough excited by laughing, singing, talking; worse lying on right side. During day, with copious green, sweetish, expectoration. Chest feels sore. Chest feels weak; can hardly talk. Influenzal cough from noon to midnight with scanty expectoration. Respiration short, oppressive; stitches in left side when breathing and lying on same side. Phthisis mucosa. Hectic fever. Severe debility. Colics. Exhausting night-sweats, especially towards morning. Hectic. Perspiration, principally on forehead and nape of neck; debilitating; smelling musty or offensive.
Bacilinium
Bacillinum is especially indicated for lungs of old people, with chronic catarrhal condition and enfeebled pulmonary circulation, attacks of suffocation at night with difficult cough. Suffocative catarrh. Tubercular meningitis. Chest oppression. Catarrhal dyspnoea. Humid asthma. Bubbling rales and mucopurulent expectoration.Favors falling off of tartar of teeth. Constant disposition to take cold. Abdominal pains, enlarged glands in groins, tabes mesenterica. Sudden diarrhoea before breakfast. Obstinate constipation, with offensive flatus. Ringworm; pityriasis. Eczema of eyelids. Glands of neck enlarged and tender.
Psorinum
Debility, independent of any organic disease, especially the weakness remaining after acute disease. Lack of reaction, i.e, phagocytes defective; when well-chosen remedies fail to act. Scrofulous patients. Dry, hard cough, with great weakness in chest. Secretions have a filthy smell. Profuse sweating. Eyes agglutinated. Blepharitis. Chronic ophthalmia, that constantly recurs. Tongue, gums ulcerated; tough mucus of foul taste adheres to soft palate.
Tonsils greatly swollen; painful swallowing, with pain in ears. Profuse, offensive saliva; tough mucus in throat. Recurring quinsy. Eradicates tendency to quinsy. Hawking up of cheesy, pea-like balls of disgusting smell and taste.
Mucous, bloody, excessively fetid, dark fluid. Hard, difficult stool, with blood from rectum and burning piles. Constipation of infants, in pale, sickly scrofulous children.
Leucorrhoea fetid, lumpy, with much backache and debility. Mammae swollen and painful. Pimples oozing an acrid fluid that burns and excoriates the glands.
Weakness of joints. Eruption around fingernails. Fetid foot-sweats. Skin dirty, dingy look. Dry, lusterless, rough hair. Intolerable itching. Herpetic eruptions, especially on scalp and bends of joints with itching; worse, from warmth of bed. Enlarged glands. Sebaceous glands secrete excessively; oily skin. Indolent ulcers, slow to heal. Eczema behind ears. Crusty eruptions all over. Urticaria after every exertion. Pustules near fingernails.
Spongia Tosta
Tubercular diathesis. Respiration short, panting, difficult. Irrepressible cough from a spot deep in chest, as if raw and sore. Chest weak; can scarcely talk. Laryngeal phthisis. Goitre, with suffocative spells. Bronchial catarrh, with wheezing, asthmatic cough, worse cold air, with profuse expectoration and suffocation; worse, lying with head low and in hot room. Oppression and heat of chest, with sudden weakness.
Swelling and induration of glands; also exophthalmic; cervical glands swollen with tensive pain on turning head, painful on pressure; Goitre. Itching; measles
Phosphorus
Inflammation and degeneration of mucus membrane. Larynx very painful. Sweetish taste while coughing. Hard, dry, tight, racking cough. Congestion of lungs. Burning pains, heat and oppression of chest. Tightness across chest; great weight on chest. Sharp stitches in chest; respiration quickened, oppressed. Much heat in chest. Pneumonia, with oppression; worse, lying on left side. Whole body trembles, with cough. Sputa rusty, blood-colored, or purulent. Tuberculosis. Repeated haemoptysis.
Adynamic with lack of thirst, but unnatural hunger. Hectic, with small, quick pulse; viscid night-sweats. Stupid delirium. Profuse perspiration. Liver congested. Acute hepatitis. Fatty degeneration. Jaundice. Little ulcer outside of large ones. Petechiae. Ecchymosis. Purpura hemorrhagica. Scurvy. Fungus haematodes and excrescences.
Do not advise it too low or too frequently, it may hasten the destructive degeneration of tubercular masses.
China Officianalis
Cannot breathe with head low. Labored, slow respiration; constant choking. Suffocative catarrh; rattling in chest; violent, hacking cough after every meal. Haemorrhage from lungs. Dyspnoea, sharp pain in left lung. Asthma; worse damp weather. Pains in limbs and joints. Indurated glands; scrofulous ulcers and caries. Stool undigested, frothy, yellow; painless. Tympanitic abdomen. Pain in right hypochondrium. Gall-stone colic (Triumfetta semitriloba). Liver and spleen swollen and enlarged. Jaundice. Internal coldness of stomach and abdomen. Gastro-duodenal catarrh.
Aclipto Indica
This medicine have a marked action on the alimentary canal and respiratory organs. It is indicated in incipient phthisis, with hard, racking cough, bloody expectoration, arterial haemorrhage, but no febrile disturbance. Very weak in the morning, gains strength during day. Progressive emaciation. All pathological haemorrhages having notably a morning aggravation.Cough dry, hard, followed by haemoptysis; worse in morning and at night. Constant and severe pain in chest. Blood bright red and not profuse in morning; dark and clotted in afternoon. Pulse soft and compressible. Burning in pharynx, oesophagus, and stomach.
Jaundice. Burning in intestines. Spluttering diarrhoea with forcible expulsion of noisy flatus, bearing down pains and tenesmus. Rumbling distention, and griping pain in abdomen. Rectal haemorrhage. Itching and circumscribed furuncle-like swellings.
Iodum
All glandular structures, respiratory organs, circulatory system are especially affected. Acute exacerbation of chronic inflammation. Acts prominently on connective tissue. The plague. Goitre. Abnormal vasoconstriction, capillary congestion followed by oedema, ecchymosis, haemorrhages, and nutritive disturbances are the pathological conditions at the basis of its symptomatology. Acute catarrh of all mucous membranes, rapid emaciation, notwithstanding good appetite, and glandular atrophy call for this remedy, in numerous wasting diseases and in scrofulous patients. Acute affections of the respiratory organs. Pneumonia, rapid extension, blood-streaked sputum. Pneumonia. Glands enlarged. Liver and spleen sore and enlarged. Jaundice. Mesenteric glands enlarged. Pancreatic disease. Flushes of heat all over body. Marked fever, restlessness, red cheeks, apathetic. Profuse sweat.
Calcarea Carb
Incipient phthisis (Ars jod; Tuberculin). It covers the tickling cough, fleeting chest pains, nausea, acidity. Tickling cough troublesome at night, dry and free expectoration in morning. Bloody expectoration. Extreme dyspnoea. Painless hoarseness. Fever with sweat. Pulse full and frequent. Chilliness and heat. Partial sweats. Night sweats, especially on head, neck and chest. Skin unhealthy; readily ulcerating; flaccid. Small wounds do not heal readily. Glands swollen.
Drosera
Spasmodic, dry irritative cough, like whooping-cough, the paroxysms following each other very rapidly. Scarcely breathe; chokes. Cough very deep and hoarse; worse, after midnight; yellow expectoration, with bleeding from nose and mouth; retching. Deep, hoarse voice; hoarseness; laryngitis. Rough, scraping sensation deep in the fauces and soft palate. Sensation as if crumbs were in the throat. Laryngeal phthisis (tuberculosis), with rapid emaciation. Harassing and titillating cough in children-not at all through the day, but commences as soon as the head touches the pillow at night. Clergyman’s sore throat, with rough, scraping, dry sensation deep in the fauces; voice hoarse, deep, toneless, cracked, requires exertion to speak. Asthma when talking, with contraction of the throat at every word uttered. Pains about hip-joint. Tubercular glands.
Kali Carbonicum:max_bytes(150000):strip_icc()/VWH-DermNetNZ-LupusVulgaris-01-0a443495e911426f98d32b6065705cc7.jpg)
Fleshy aged people, with dropsical and paretic tendencies. Sweat, backache, and weakness. Throbbing pains. Tendency to dropsy. Tubercular diathesis. Cutting pain in chest. Hoarseness and loss of voice. Dry, hard cough, with stitching pains and dryness of pharynx. Bronchitis, whole chest is very sensitive. Expectoration scanty and tenacious. Hydrothorax. Leaning forward relieves chest symptoms. Expectoration must be swallowed; cheesy taste; copious, offensive, lump. Coldness of chest. Wheezing. Cough with relaxed uvula. Tendency to tuberculosis; constant cold taking; better in warm climate.
Flatulence. Dyspepsia. Epigastrium sensitive externally. Easy choking when eating. Epigastric pain to back. Stitches in region of liver. Old chronic liver troubles, with soreness. Jaundice and dropsy. Distention and coldness of abdomen. Pain from left hypochondrium through abdomen; must turn on right side before he can rise.
Syphilinum
When Tuberculinum fails Syphilinum often follows advantageously, producing a reaction. Diseased cartilages of larynx. Pain and oppression at bifurcation of bronchi and in larynx. Attacks of chronic spasmodic bronchial asthma, dyspnoea, wheezing and rattling of mucus. Hard, constant cough, with thick, yellow or greenish, tasteless expectoration or dry, racking cough, with thick, purulent expectoration. Prostration and debility. Chest pain.
Ferrum Aceticum
Epistaxis; especially adapted to thin, pale, weak children who grow rapidly and are easily exhausted; varices of the feet; copious expectoration of greenish pus; asthma; worse, sitting still and lying; phthisis, constant cough, vomiting of food after eating, haemoptysis.
Ferrum Met
Hot breath.-Oppressed, short breathing.-Hoarseness and roughness in the throat. Purulent expectoration. Spasmodic cough, with expectoration of tenacious and transparent mucus or dry spasmodic cough, commencing with vomiting of food. Fetid, greenish expectoration, with streaks of blood.
Difficulty of respiration, with almost imperceptible rising of the chest, and great dilation of the nostrils during expiration. Fullness and tightness of the chest. Asthma (after midnight), Asthma most violent when lying, or when sitting still without doing anything. Fits of suffocation. Burning pain in the throat and the upper part of the body, and coldness in the extremities. Constrictive oppression of the chest. Constrictive spasms in the chest. Stitches and soreness in the chest. Tensive lancinations in the chest, extending to the shoulder-blades. Congestion in the chest.
Inflation and hardness of the abdomen. Liver enlarged, sensitive. Spleen large, sore. Cramps in spleen region. Camps. Colics. Watery and corrosive diarrhoea, sometimes accompanied by cramp-like pains and colic.
Sanguinaria Canadensis
Edema of larynx. Trachea sore. Heat and tension behind the sternum. Aphonia. Cough of gastric origin. Cough, with burning pain in chest. Sputum tough, rust-colored, offensive, almost impossible to raise. Spasmodic cough after influenza and after whooping-cough. Tickling behind sternum, causes a constant hacking cough. Burning soreness chest, through the shoulder. Haemoptysis. Severe dyspnoea and constriction of chest. Offensive breath and purulent expectoration. Burning in chest. Fibroid phthisis. Pneumonia. Asthma with stomach disorders. Valvular disease with lung development, phosphates in urine and loss of flesh. Sudden stoppage of catarrh of air passages brings on diarrhoea.
Burning, vomiting. Nausea, with salivation. Sinking, faint all-gone feeling (Phos; Sep). Spitting up of bile; gastro-duodenal catarrh.
Abdomen: Diarrhoea as coryza improves. Pain over region of liver. Diarrhoea; bilious, liquid, gushing stool. Cancer of rectum.
Silicea
Colds fail to yield; sputum persistently muco-purulent and profuse. Slow recovery after pneumonia. Cough and sore throat, with expectoration of little granules like shot, which, when broken, smell very offensive. Cough with expectoration in day, bloody or purulent. Stitches in chest through to back. Violent cough when lying down, with thick, yellow lumpy expectoration; suppurative stage of expectoration. Pain or painful cold feeling in abdomen, better external heat. Hard bloated. Colic; cutting pain, with constipation; yellow hands and blue nails. Rumbling in bowels. Inguinal glands swollen and painful. Hepatic abscess. Boils on gums. Abscess at root of teeth. Pyorrhea. Caries of mastoid.
Complications of tuberculosis
Although some people may develop no complications, others range from mild to severe complications, including death. Some of the more severe complications include lung function damage, bone pain (spine, ribs, and joints), meningitis, kidney and/or liver malfunction, cardiac tamponade, and visual disturbances.
P. S : This article is only for doctors having good knowledge about Homeopathy and allopathy, for learning purpose(s).
For proper consultation and treatment, please visit our clinic.
Location, address and contact numbers are given below.
NoN of above mentioned medicine(s) is/are not the full/complete treatment, but just hints for treatment; every patient has his own constitutional medicine along with these mentioned above.
To order medicine by courier, please send your details at WhatsApp– +923119884588
 Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS) ; senior research officer Dnepropetrovsk state medical academy Ukraine; is a leading Homeopathic physician practicing in Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Dr. Sayyad Qaisar Ahmed (MD {Ukraine}, DHMS) ; senior research officer Dnepropetrovsk state medical academy Ukraine; is a leading Homeopathic physician practicing in Al-Haytham clinic, Umer Farooq Chowk Risalpur Sadder (0923631023, 03119884588), K.P.K, Pakistan.
Find more about Dr. Sayyad Qaisar Ahmed at :
https://www.youtube.com/Dr Qaisar Ahmed